

This heretical investigation shows the anatomy of medical democide inflicted upon an unwitting American people under the rubric of the so-called global pandemic. The mass execution of patients with courses of an alleged anti-viral drug, remdesivir — occurred under the direction of health officials.
Steve ‘Snoopman’ Edwards proves that US health officials and the drug’s manufacturer, Gilead Pharmaceuticals, knew that remdesivir caused multiple organ failure, including impairing kidney function, before the U.S. Food and Drug Administration’s emergency use authorization of May 1 2020.
By Steve ‘Snoopman’ Edwards
➼ Step 1: Select the Most Lethal Drug for a Live Global Simulation

At the beginning of May 2020, when the Food and Drug Administration issued an Emergency Use Authorization (EUA) to permit administering of an experimental drug for the treatment of hospitalized Covid-19 adults and children — many hospitals across the United States of America became mechanisms of state-sanctioned mass murder, or democide.
Democide is defined by R.J Rummel in his 1994 book, Death by Government, as state-sanctioned murder of any domestic person, or civilian people by government officials, who act with the approval of the highest officials or state policy, whether explicitly or implicitly, and includes genocide, politicide and mass murder.
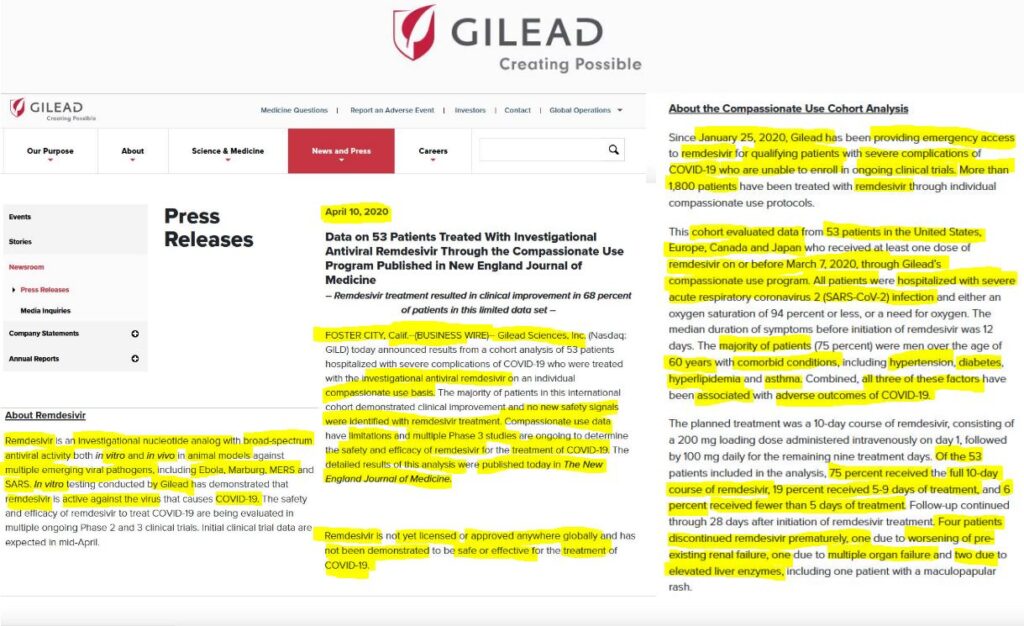
The drug, remdesivir — which is marketed as Veklury — was previously made available on ‘compassionate use’ grounds for over 1800 coronavirus patients from January 25 2020 in the United States, according to an April 10 2020 press release by pharmaceutical manufacturer, Gilead Sciences Inc.i

Shockingly, Gilead’s ‘compassionate use’ rhetoric was packaged with sinister weaponized ironic humor, because the company knew the drug’s lethality, as this study will show. Indeed, remdesivir stood out as the only drug that killed over half of the humans in its cohort, during a four-drug trial during 2019, ostensibly conducted to combat an Ebola virus outbreak in the African Republic of Congo.
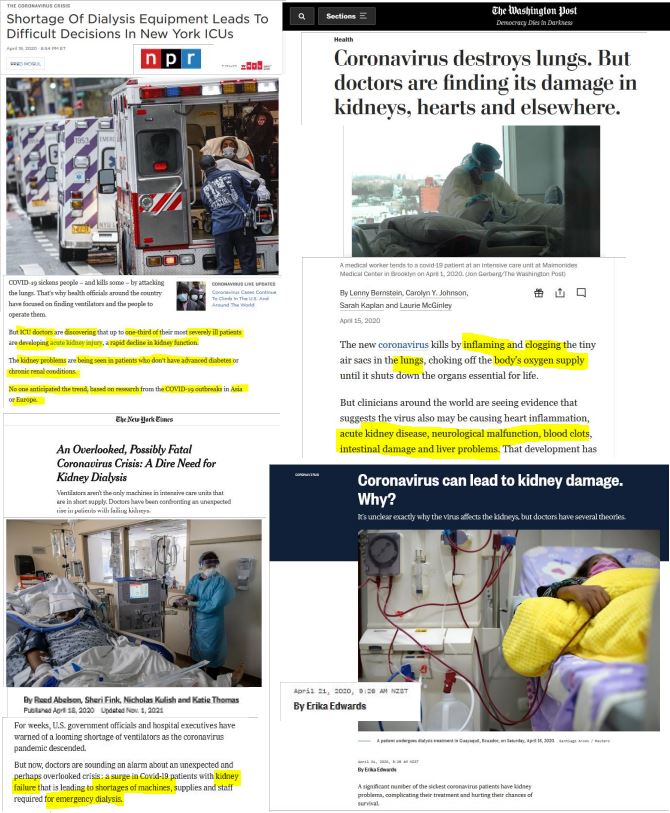
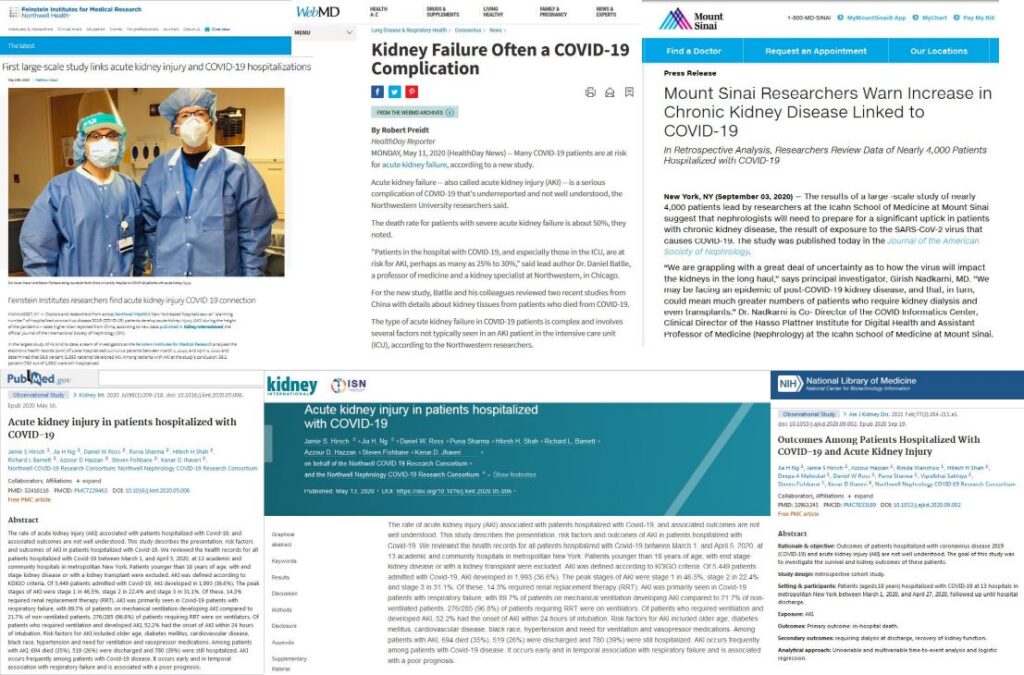
One U.S. doctor’s curiosity was aroused when he noticed from mid-May 2020, numerous doctors in New York all remarking in the public media that they had never seen a respiratory virus cause kidney failure.iii
The medical doctor, Bryan Ardis, wondered what drugs the doctors were prescribing to hospitalized Covid-19 patients, and he found it was remdesivir.
He had never heard of the drug.
Dr Ardis — who founded what became the North Texas Healing Centerii — looked up the US National Institutes of Health website to learn about remdesivir. The NIH website cited the trial in the Congo to treat Ebola virus, and Dr Ardis saw the medication was distinguished for having the highest mortality rate among the four drugs trialed without a proper control group given placebo treatment.
Another study, which also lacked a control group, was a 28-day remdesivir trial with 53 Covid-19 patients in which 13% of the patients died. Both trials involving remdesivir were published in The New England Journal of Medicine.
Since May 2020, Dr Bryan Ardis — who founded what became the North Texas Healing Centerii — has been sounding the alarm that remdesivir causes multiple organ failure, including kidney (renal) failure, which results in the body’s waste water flooding the lungs, causing pulmonary edema.
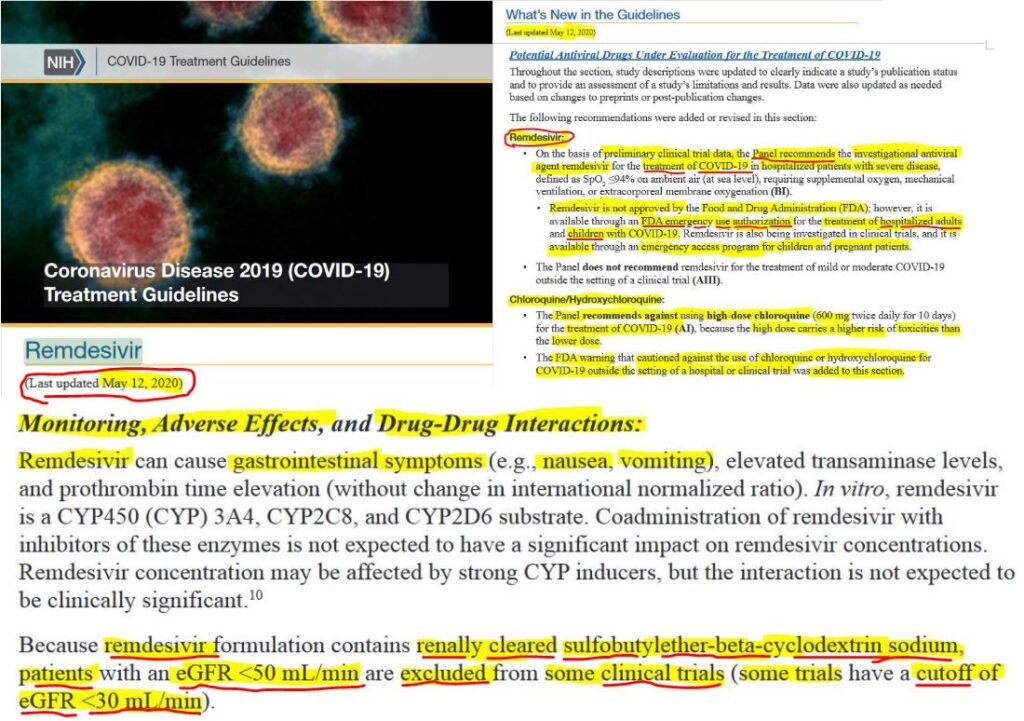
Crucially, remdesivir contains an inactive solubilizing agent, or excipient, called sulfobutylether-β-cyclodextrin (SBECD), which can accumulate in patients with impaired renal function, since it is excreted through kidney filtration. SBECD is a sodium salt substance known to improve the aqueous solubility and dissolution rates of therapeutic agents. The Duke University School of Medicine’s Duke Antimicrobial Stewardship Outreach Network (DASON) pointed out in an article entitled, “Cyclodextrin and Renal Function”, that SBECD may accumulate in patients with renal impairment. The DASON medical group stated in their article, which was reviewed 15 December 2020, added that SBECD may further potentiate the risk for nephrotoxicity, or a poisonous effect in the kidneys, with the potential risk increasing with total dose and level of renal impairment.
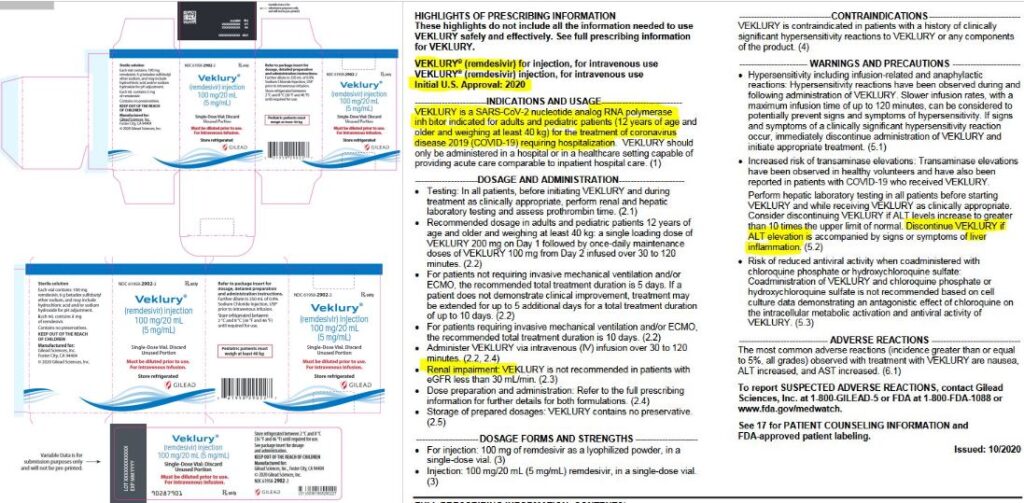
As I show in the subsection “Alphabet Health Agencies, Gilead & Fauci et al Play Contrived Ignorance”, Gilead’s product sheet for Veklury — which was published by the FDA on October 22 2020 — stated in the prescribing information that the “excipient betadex sulfobutyl ether sodium is renally cleared and accumulates in patients with decreased renal function”.
Moreover, the U.S. National Institutes of Health were aware that remdesivir’s solubilizing agent, SBECD, had the potential to cause severe adverse events in patients with acute kidney disease before the health agency’s COVID-19 Treatment Guidelines Panel recommended the medication for hospitalized Covid-19 patients with severe disease, in May 2020.
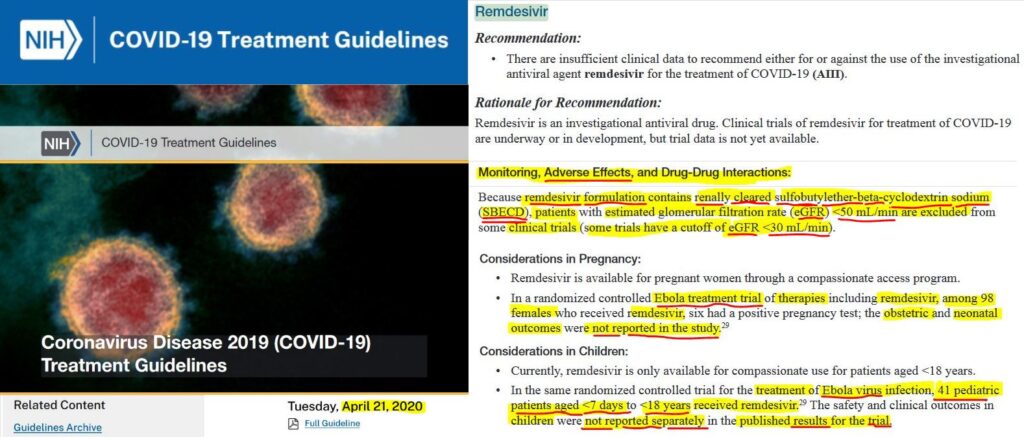
This means that in April 2020, the U.S. National Institutes of Health (NIH) were well aware of the co-morbidity danger to patients with poor kidneys and deemed to be afflicted Covid-19, if they were to be treated with remdesivir, since it contained the solubizing agent, SBECD, a sodium salt.
In May 2020, when NIH’s COVID-19 Treatment Guidelines Panel recommended remdesivir for hospitalized Covid-19 patients with severe disease over Ivermectin, Chrlorquine and Hydroxychloroquine, this board of scientists, doctors and health officials minimized the risk of toxicity to such patients with impaired kidneys. Severe renal impairment is measured at eGFR < 30 mL/min, or an estimated glomerular filtration rate of under 30 milliliters per minutes.
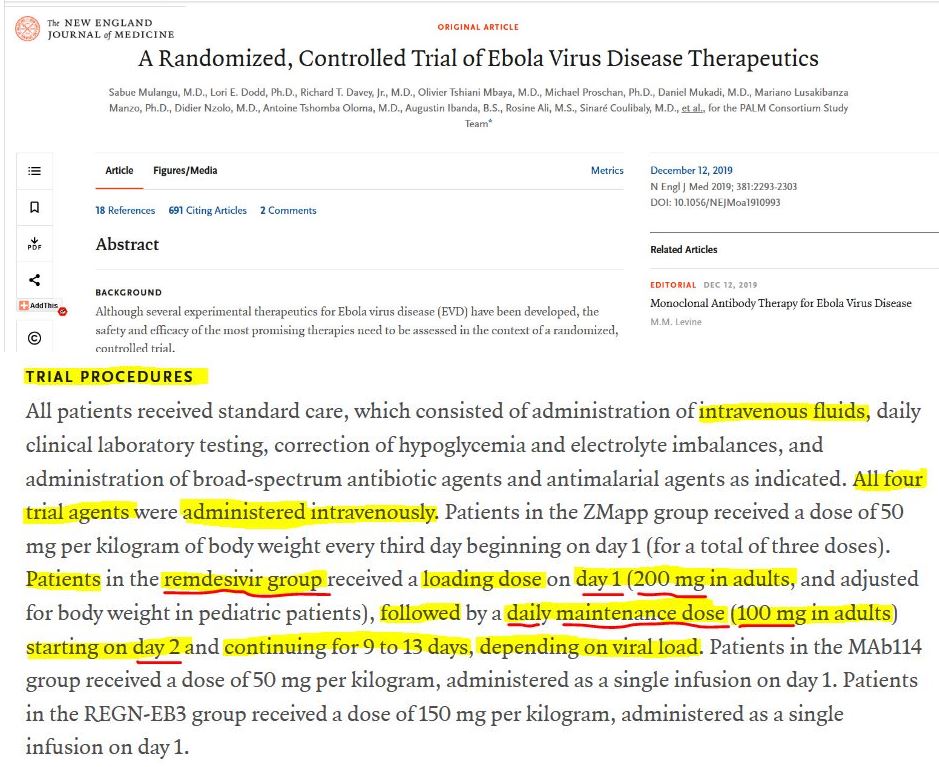
The doses recommended by NIH’s COVID-19 Treatment Panel were the same/or similar as the dosage levels administered to the remdesivir group in the National Institute of Allergy and Infectious Diseases (NIAID)-sponsored Ebola Drug trial.
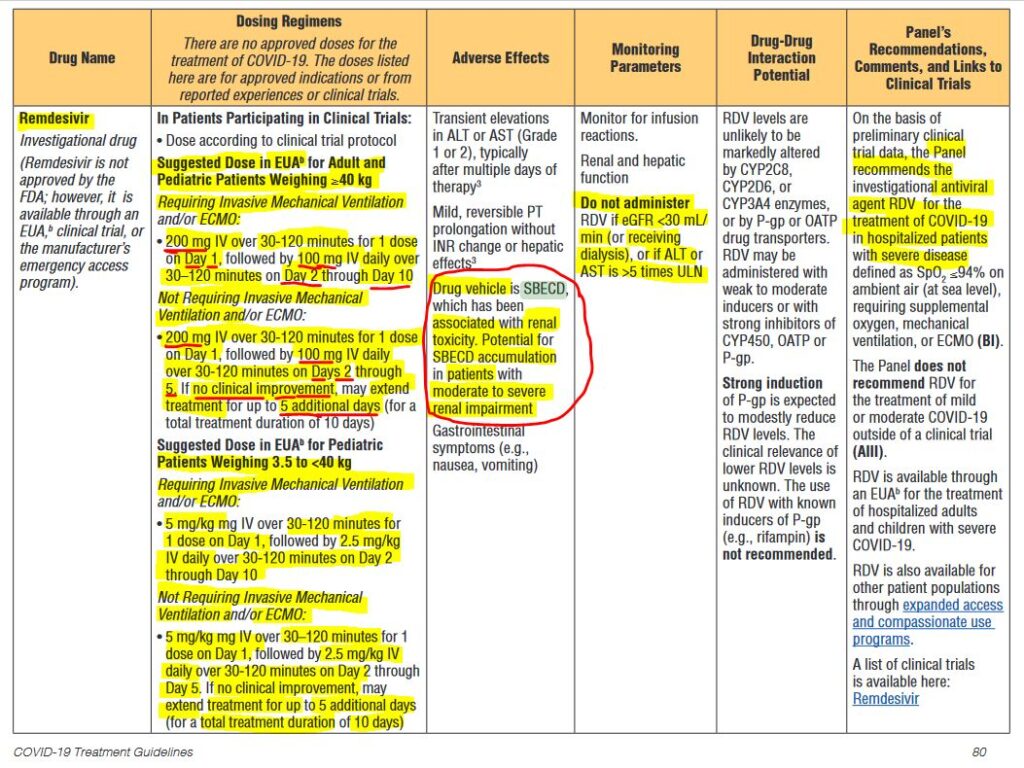
The NIH’s suggested course of remdesivir was one 200mg dose on day 1, followed by 100mg daily dose from days 2 to 10, by intravenous injection over periods of 30 to 120 minutes for Covid-19 adult and child patients weighing 40 kilograms, or more, who required invasive mechanical ventilation and/or extracorporeal membrane oxygenation (ECMO), which pumps oxygen-filled blood to tissues in the body.
For such patients not requiring invasive mechanical ventilation and/or ECMO, the NIH’s suggested course of remdesivir was one 200 mg dose over 30 to 120 minutes on Day 1, followed by 100 mg daily doses over 30 to120 minutes on Days 2 through 5. If there was no clinical improvement, hospitals were advised to extend the treatment for up to 5 additional days (for a total treatment duration of 10 days).
The dosing regimens section on page 81 and 82 of this May 12th 2020 NIH advisory were the only places in the 124 page document that mentioned remdesivir contains the sulfobutylether-β-cyclodextrin (SBECD) and that it is associated with renal toxicity and has the potential to cause severe renal impairment. Apart from a key that elaborated what the acronym SBECD meant, there was no further information in the document warning that the recommended dosing regimen was the same/or similar to that used in the Ebola drug trial, in which 53% of the remdesivir cohort died.
To find that out, hospital administrators, doctors and nurses would have had to read the Ebola study in The New England Journal of Medicine cited at the end of the Remdesivir secton of “Potential Antiviral Drugs Under Evaluation for the Treatment of COVID-19” on page 46 — amid an alleged global pandemic.
Or, they would have had to have found Singh et al’s study “Remdesivir in COVID-19: A critical review of pharmacology, pre-clinical and clinical studies”, which not only noted that remdesivir group’s mortality rate was significantly worse than the best performing drug in the Ebola trial.
Singh et al’s paper, which was published in the July-August 2020 edition of the US National Library of Medicine National Institutes of Health, also made the observation that 23% of patients, in a subsequent remdesivir trial to test the drug’s efficacy in treating Covid-19 patients, suffered three types of serious adverse events: acute kidney injury, septic shock, and multi-organ failure. The study, entitled “Compassionate Use of Remdesivir for Patients with Severe Covid-19”, which was published in The New England Journal of Medicine on April 10 2020, was used by the US National Institutes of Health, the National Institute of Allergy and Infectious Diseases and the Food and Drug Administration to justify its emergency use.
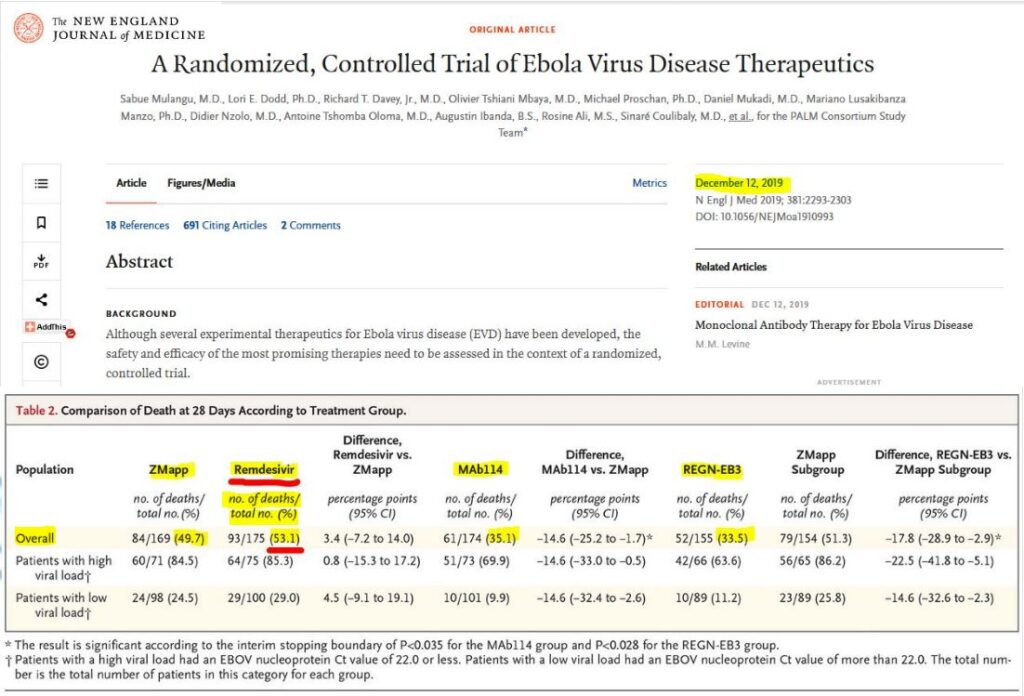
The NIH’s April and May 2020 advisory’s produced by the COVID-19 Treatment Guidelines Panel, cited a study entitled “A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics” that was published in The New England Journal of Medicine on December 12 2019. Adults in the Remdesivir Group of this Ebola drug trial received one 200 mg dose intravenously on day one, followed by 100 mg daily doses from day 2 through to day 9 to 13, depending on the viral load.
Therefore, the remdesivir dosing regimes between the Ebola drug trial and those recommended for Covid-19 patients were equivalent.
Amid the Covid-19 emergencies, many New York hospital ICU rooms placed patients on ventilators because people were drowning in excess water that had seeped into the lungs from this drug-induced kidney failure. A critical demand for dialysis machines ensued, heightening the pressure on ICU’s to manage limited resources.
Dr Ardis stated the misdiagnosed phenomena has become known as ‘Covid Pneumonia’, and the term masks the ongoing mass murder occurring under the rubric of the ‘Covid-19 Pandemic’.
In addition to renal failure, the drug can also causes multiple organ failure, including lung failure and heart failure, as numerous subsequent studies published in various medical journals have shown.iv
Remdesivir was one of four drugs trialed during the Ebola outbreak in 2019 in the African Republic of Congo and was the most lethal, killing 53% of patients in its cohort of 175 people.
Director of the National Institute of Allergy and Infectious Diseases, Dr Anthony Stephen Fauci — who is also the Chief Medical Advisor to the U.S. President — could not have been unaware of the drug’s lethality. After all, the trial’s second highest mortality group, ZMapp — which tallied 49.7% of its patient cohort — received funding as an drug to treat Ebola Zaire in 2014 from the Defense Threat Reduction Agency (DTRA) within the Department of Defense and the National Institute of Allergy and Infectious Diseases (NIAID) of HHS’ National Institutes of Health.
Moreover, funding for the development and manufacturing of ZMapp toward the goal of U.S. Food and Drug Administration approval, was awarded by the U.S. Department of Health and Human Services (HHS) Biomedical Advanced Research and Development Authority (BARDA), as Global Biodefense reported September 4 2014, in an article headlined, “BARDA to Rapidly Accelerate ZMapp Ebola Drug”.
Furthermore, the 2019 Ebola drug trial was primarily funded by the Fauci-controlled National Institute of Allergy and Infectious Diseases (NIAID), which is a federal agency of the U.S. National Institutes of Health, as an August 12 2019 press release from the U.S. National Institutes of Health (NIH) shows.
The Ebola trial tested four drugs, with one drug supplied by each of four pharmaceutical companies, Gilead, MappBio, Regeneron, and Ridgeback Biotherapeutics. In their review of remdesivir’s track record entitled, “Remdesivir in COVID-19: A critical review of pharmacology, pre-clinical and clinical studies”, Singh et al noted that remdesivir was less effective than other monoclonal antibodies and its mortality of 53% being significantly worse. Singh et al observed the, “Authors alluded these differences due to more sicker patients in the remdesivir arm”.
Ironically, it was the ZMapp patient cohort in the Ebola trial that was designated with control group status. In other words, the scientific method was breached, since medical experiments are supposed to have a control in which a sample population in a trial are given placebo treatment.
That MappBio’s bio-engineered proteins in the form of the triple monoclonal antibody drug, ZMapp, was deemed to be the control group, suggests a subtext was signalled by the Covid Bandits: follow the money on the map to locate the supreme Corona cliqué
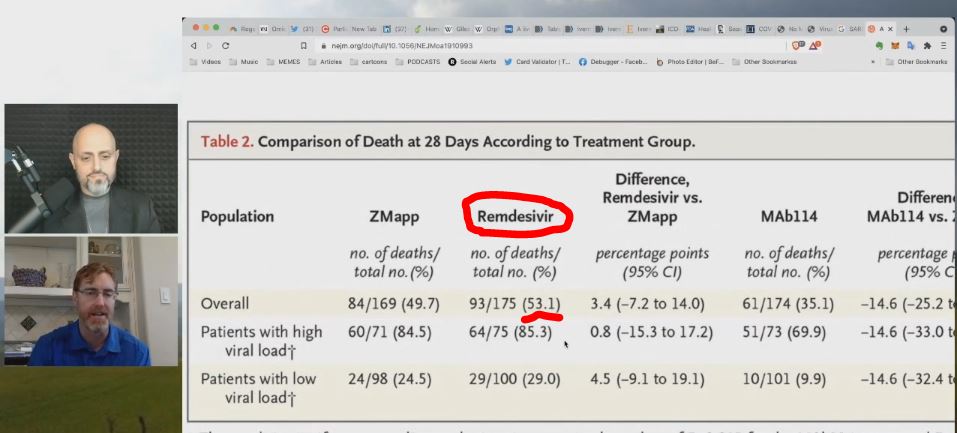
Dr Ardis said in a December 2nd 2021 interview on The Last American Vagabond, that two of the four drugs, Remedsivir and ZMapp, performed so badly, they were pulled before the trial was completed.
Crucially, the Ebola drug trial study which was published in the New England Journal of Medicine did not mention how lethal Remdesivir could be in the abstract, despite mentioning that the drugs, produced by Regeneron, and Ridgeback Biotherapeutics, performed more favorably than the drugs, ZMapp and remdesivir, with respect to mortality.
Intriguingly, the ‘Mortalilty’ subsection in the study’s main body stated there was a clear separation in the mortality data between Regeneron’s REGN-EB3 and Ridgeback’s MAb114 groups, and Gilead’s remdesivir and Mapp Biopharmaceuticals’ ZMapp.
The authors appeared to assume that the patients who died during or after treatment was due to having not recovered from the Ebola virus, rather than the therapeutic doses being too toxic. The medium time to recovery for the remdesivir group was deemed to be greater than 28 days because the mortality rate exceeded 50%. The medium recovery time for the best performing drug, REGN-EB3, was 15 days.
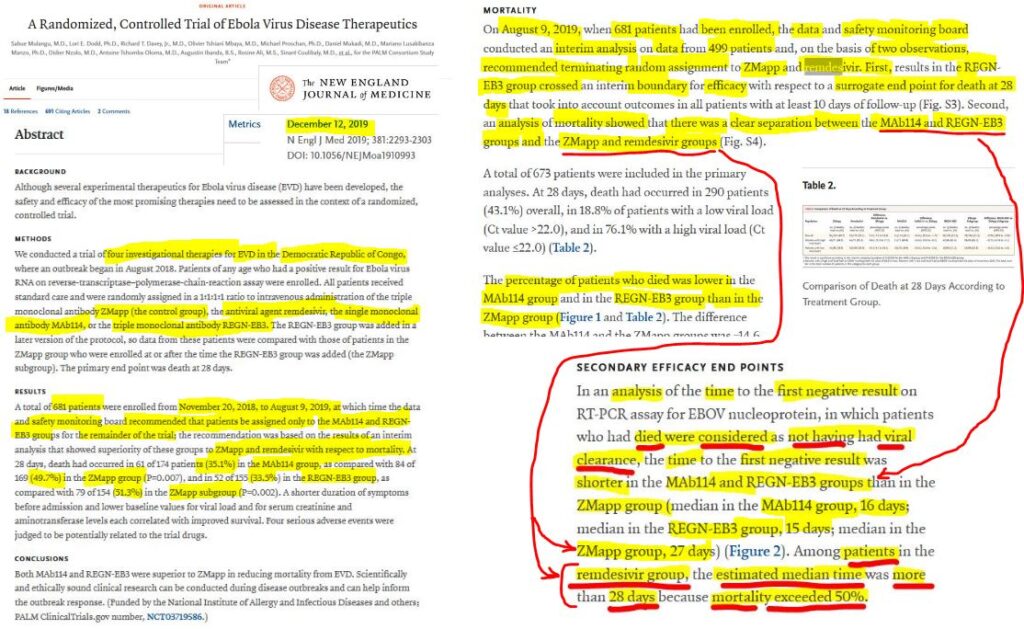
The data showing that the mortality rate in the Remdesivir cohort was 53% was stated in table 2, titled “Comparison of Death at 28 Days According to Treatment Group”.
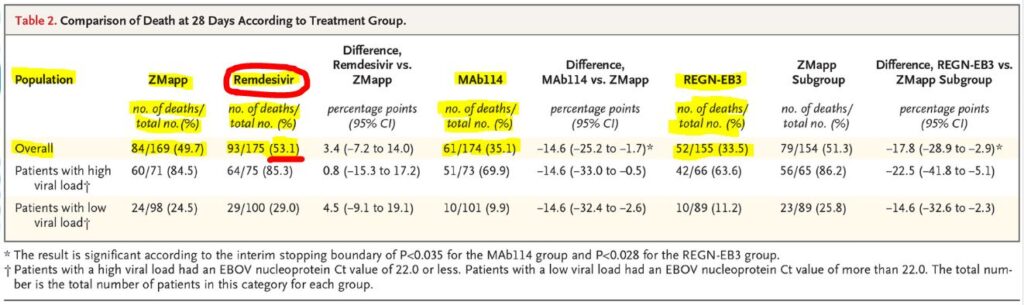
On August 12 2019, the U.S. NIH announced that an ‘independent’ Data and Safety Monitoring Board (DSMB) had called for a premature end to the Ebola drug trial, ostensibly because one of the drugs had met a trial’s protocol. The drug, REGN-EB3 produced by Regeneron, achieved the lowest fatality rate of the four drugs, killing 33% of the patients in its cohort.
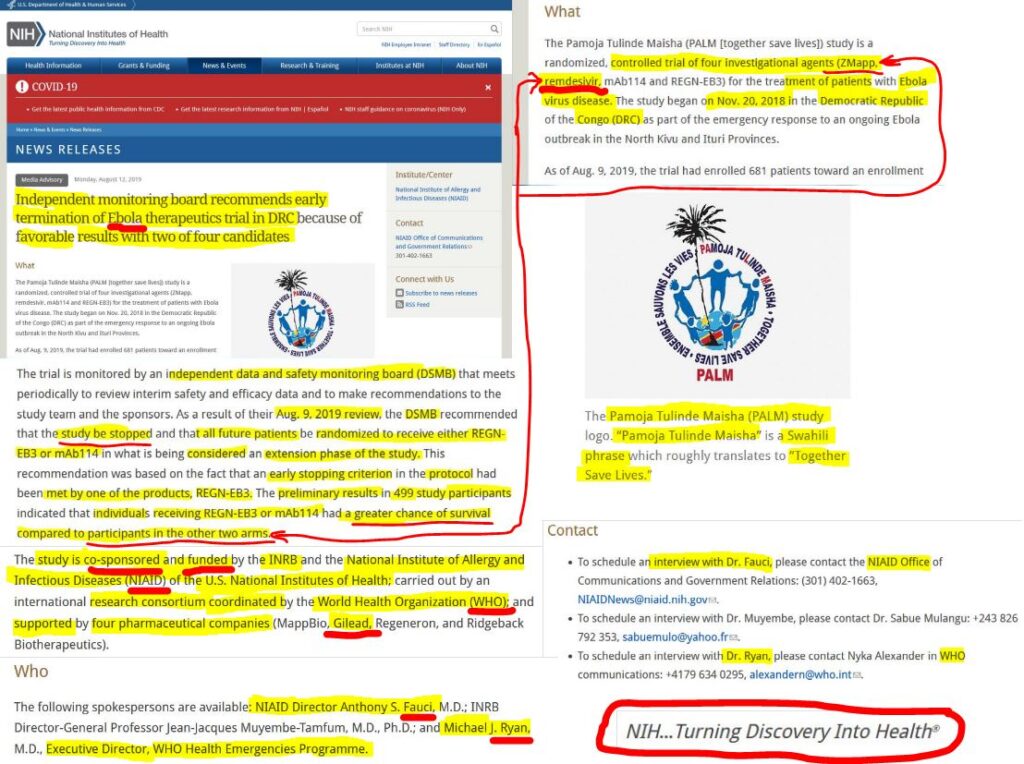
The NIH’s Ebola drug trial early termination announcement also shows that the Executive Director of WHO Health Emergencies Programme, Dr Michael J. Ryan, along with Dr Fauci, were among the three spokespeople listed in the news release communicating a halt to the Ebola drug trial. This news release — which acknowledged the research group’s speedy work amid challenging conditions in a conflict zone — was transmitted four months before the peer-reviewed findings from the Ebola drug trial were published in The New England Journal of Medicine.
As the alleged ‘global Covid-19 pandemic’ supposedly began ‘spreading’ in Wuhan City, in the Hubei Province of totalitarian China, The New England Journal of Medicine published the findings of the Fauci-controlled NIAID Ebola drug trial on December 12 2019.
The publication of this paper in The New England Journal of Medicine was like an opening salvo that reported, in effect, a beta-test of remdesivir’s field trial in an African nation.
An opening salvo, because the paper was the first of several that would embroil the prestigious publication as the alleged global pandemic unfolded.
The behaviours of The New England Journal of Medicine, under the direction of its new Editor-in-Chief, Eric J. Rubin, along with other players, were consistent with coordinated moves as performative ‘Hostage Posting Rituals’ to signal ‘cooperation’, as game theory predicts.
➼ Step 2: Short-Circuit skeptical investigations into the Great Corona Planpanic
Game theory strategies such as ‘Hostage Exchanges’ are used by nation states, international syndicates and monopolistic cartels to stabilize power structures while aggressive colluding rivals seek to construct new areas of market dominance by illegal, fraudulent and repugnant means that harm their more dynamic, innovative smaller and peaceful competitors. During the Cold War, game theory was developed to stabilize the power structures of the Soviet Russian Empire and the American-led Western Empire, to mitigate the chances that the world’s two super-powers would engage in nuclear war.
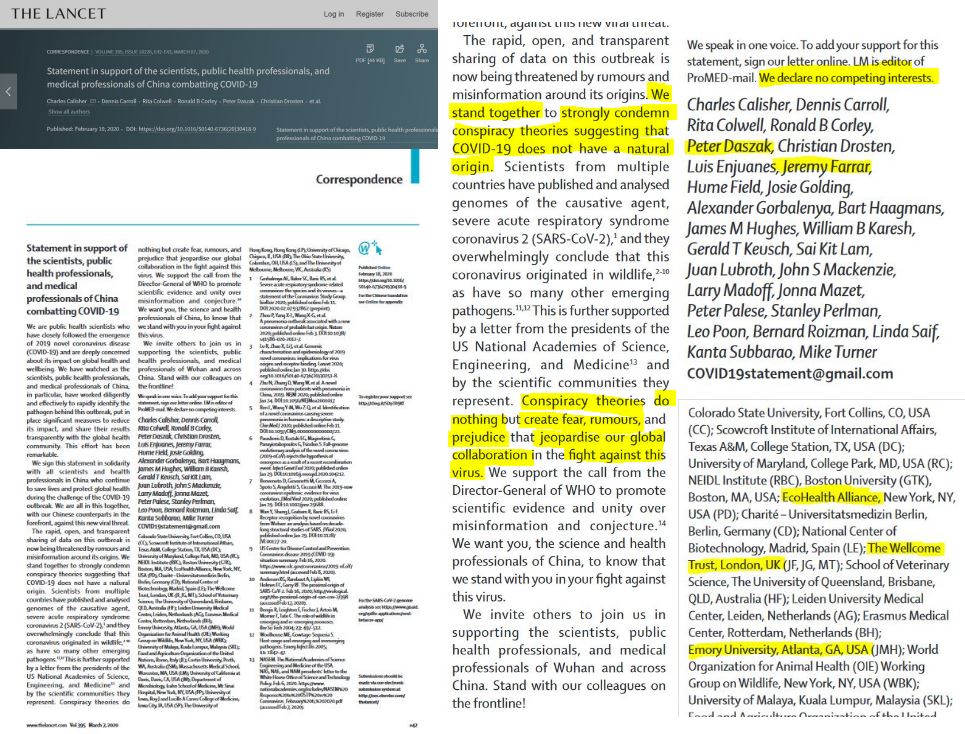
Then, on February 19, 2020, as rumours, disinformation and conspiring theories were swirling about the origins of the of the SARS-CoV-2 coronavirus outbreak, the prestigious Lancet medical journal published a statement that effectively rejected the lab-leak hypothesis — as well as a possible bio-terrorist plot — while endorsing the idea that COVID-19 had a natural origin.
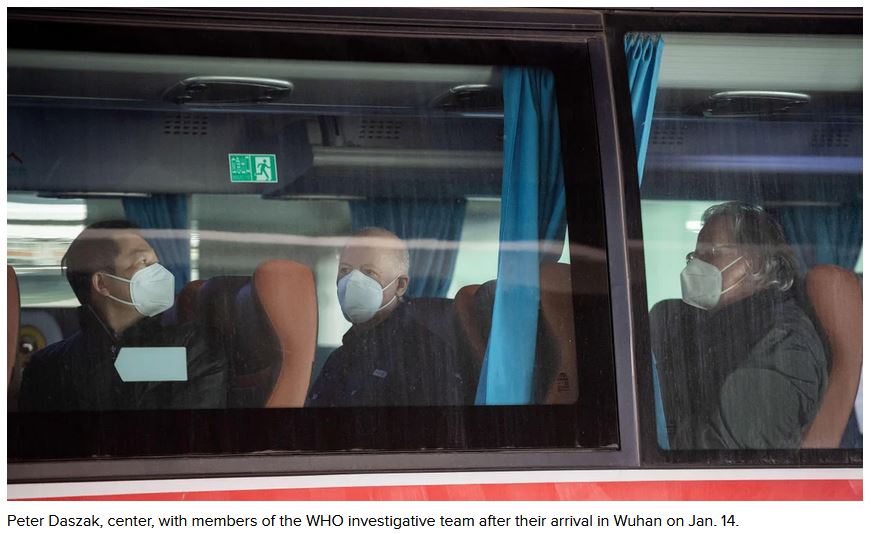
Among the signers of the statement was the President of EcoHealth Alliance, Dr Peter Daszak, who is credited elsewhere for discovering the origins of the first coronavirus outbreak, SARS-CoV-1 (November 2002-March 2003).
Ironically, the signers declared they had no competing interests. Yet, between 2008 and 2020, EcoHealth Alliance was the recipient of at least $63 million in Federal funding from the US Department of Health and Human Services, and its US National Institute of Allergy and Infectious Diseases (NIAID), as well as the Pentagon’s Defense Threat Reduction Agency (DTRA).
Indeed, beginning in 2014, Dr Peter Daszak was Principal Investigator of a six-year NIH project which was awarded to the EcoHealth Alliance and which focused on the emergence of novel zoonotic coronaviruses with a bat origin.
Crucially, in October 2014 US President Barack Hussein Obama banned ‘Gain of Function’ research on potential pandemic viruses such as avian flu, SARS and MERS amid concerns from scientists. This research could be dual purposed, to make vaccines or to weaponize pathogens.
Beginning in fiscal year 2014, the Pentagon’s Defense Threat Reduction Agency (DTRA) began awarding funding to EcoHealth Alliance for a work program labeled “Scientific Research – Combating Weapons of Mass Destruction”. By 2020, the grants totalled $33.85 million.
Between fiscal year 2008 and 2020, EcoHealth had also received $41.91 million in awards from the Pentagon, with $37.61 million granted by the Defense Threat Reduction Agency (DTRA) — meaning that 90 percent of EcoHealth’s Pentagon awards were for just one program from DTRA. Over the same period, EcoHealth Alliance was also awarded $13.17 million from the Department of Health and Human Services, as The New York Post reported July 1 2021.
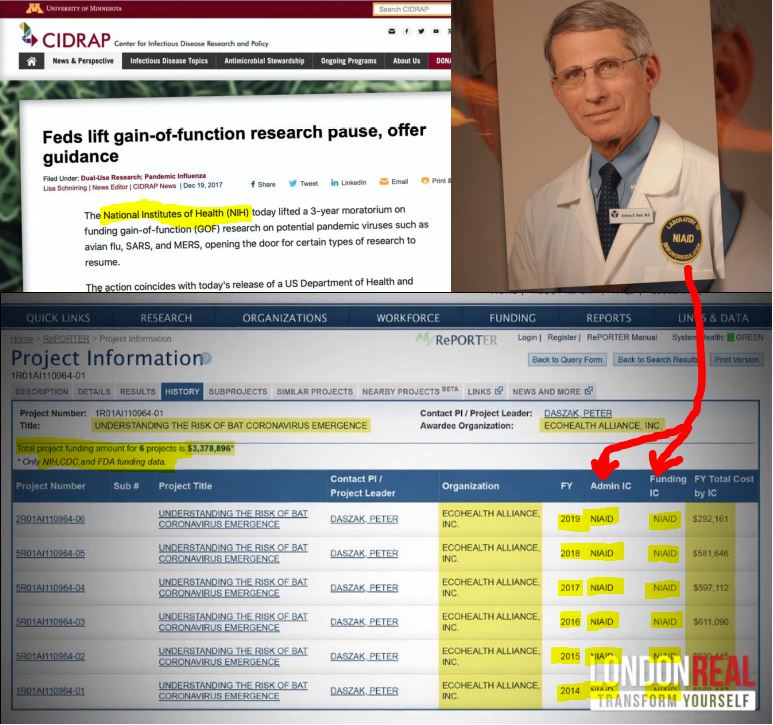
EcoHealth Alliance was also awarded $7.5 million for a project, called – “Understanding the Risk of Bat Coronavirus Emergence” from the National Institute of Allergy and Infectious Diseases (NIAID) over an 11 year period to 2020.
Dr Fauci funded this ‘Gain of Function’ research at the Wuhan Institute of Virology in two installments of $3.7 million for three-year terms, the first beginning in 2014 on Obama’s watch, and the second in 2017 on Trump’s watch.
EcoHealth Alliance was used as the funding conduit, and Peter Daszak oversaw the repackaging of monies to flow to numerous subcontracted bio-research labs, universities and medical schools.
As Vanity Fair reported June 3 2021 in an investigation entitled, “The Lab-Leak Theory: Inside the Fight to Uncover COVID-19’s Origins”:
❝The Lancet statement effectively ended the debate over COVID-19’s origins before it began.❞
According to the Lancet, Daszak moved quickly to snuff out a lab-leak theory because if such an origin took hold, it could have mired the field indefinitely in moratoriums and funding restrictions. To support this lab-leak framing, Vanity Fair interviewed over 40 people, including the author of Hacking Darwin: Genetic Engineering and the Future of Humanity, Jamie Metzl. He told Vanity Fair what he thought was Daszak’s motivation for organizing the Lancet statement: “If zoonosis was the origin, it was a validation … of his life work …. But if the pandemic started as part of a lab leak, it had the potential to do to virology what Three Mile Island and Chernobyl did to nuclear science.”
But, was that all there was to Dr Daszak’s motive?
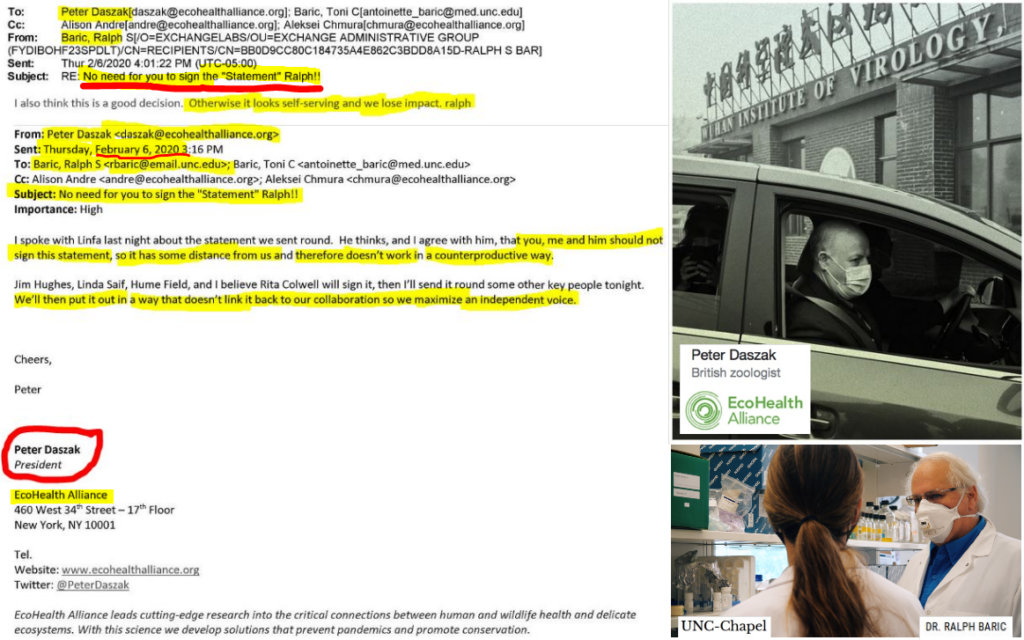
It turns out that Dr Daszak, a zoologist, had not only concealed his role as the key organizer behind the Lancet statement. Dr Daszak also ensured that one of his associates, Professor Ralph S. Baric of the University of North Carolina Chapel Hill campus, did not sign The Lancet statement, in order to create “some distance” to hide their “collaboration”.
In a 6 February 2020 email, subject-lined, “No need for you to sign the “statement” Ralph!!”, Dr Daszak told Dr Baric that we’ll put out the natural outbreak origins statement in a way that “doesn’t link back to our collaboration so we maximize an independent voice.”
Matthew F. Pottinger, United States Deputy National Security Advisor (2019- 2021) who had approved a COVID-19 origins team in early 2020, run by the NSC directorate, stated that many leading experts had either received or approved funding for gain-of-function research. Pottinger told Vanity Fair that their “conflicted” status meant they “played a profound role in muddying the waters and contaminating the shot at having an impartial inquiry.”
The US National Security Council Directorate inquiry was subsequently shutdown.
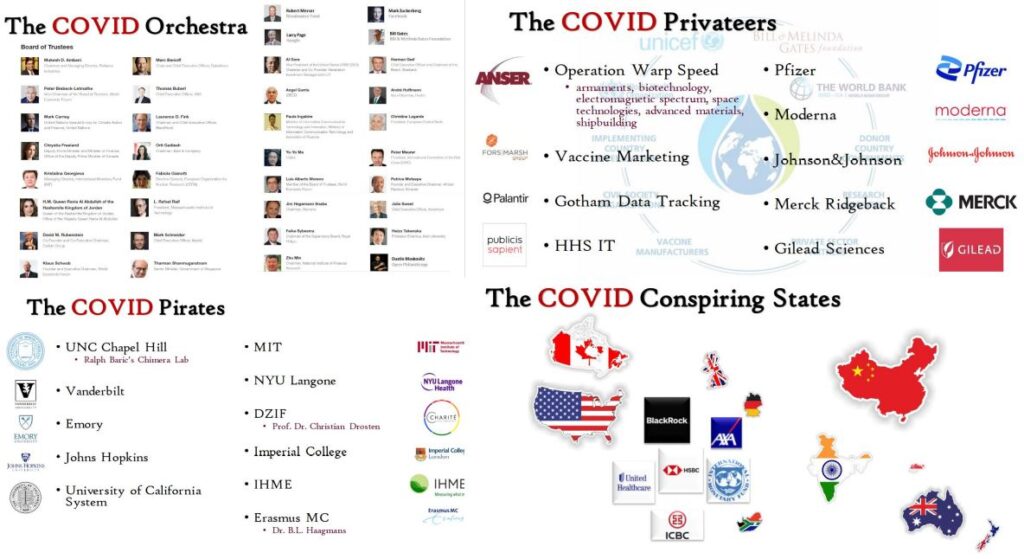
Yet, Vanity Fair regarded the idea of a bio-terrorist plot with a weaponized pathogen as a wing nut Alt-right conspiracy theory. While the Vanity Fair investigation reported that Dr Daszak had repackaged NIH funding through a myriad of subcontracted studies — which created a code of silence, or Omertà, about the gain of function lab work into the coronavirus — the magazine omitted the deep state élite connectivity to EcoHealth Alliance.
The EcoHealth Alliance’s extensive partners include: the US Centers for Disease Control and Prevention (CDC), John Hopkins University Bloomberg School of Public Health, the United Nations (FAO) Food and Agriculture Organization and Johnson & Johnson. Among the science advisors to the EcoHealth Alliance are Dr. Scott Dowell, who is the Deputy Director for Surveillance and Epidemiology at the Bill & Melinda Gates Foundation, and Captain Jason Thomas, who is the Biosurveillance Coordinator at the CDC’s Center for Surveillance, Epidemiology, and Laboratory Services (CSELS).
With questions growing in mid-2021, NIH director Dr. Francis Collins released a statement on May 19 asserting that “neither NIH nor NIAID have ever approved any grant that would have supported ‘gain-of-function’ research on coronaviruses that would have increased their transmissibility or lethality for humans.”
However, in a June 2021 interview with Fox News, former CDC director Dr. Robert Redfield (2018-2021), supported the lab-leak theory from Wuhan. Redfield — who co-founded the University of Maryland’s Institute of Human Virology — said an “an alternative hypothesis” was that the bat virus was taught, educated, and evolved in a laboratory to “efficiently transmit human to human.”
From the outset, Professor Ralph Baric’s work appeared to be focussed on making the coronavirus pathogenic to human lung tissue.
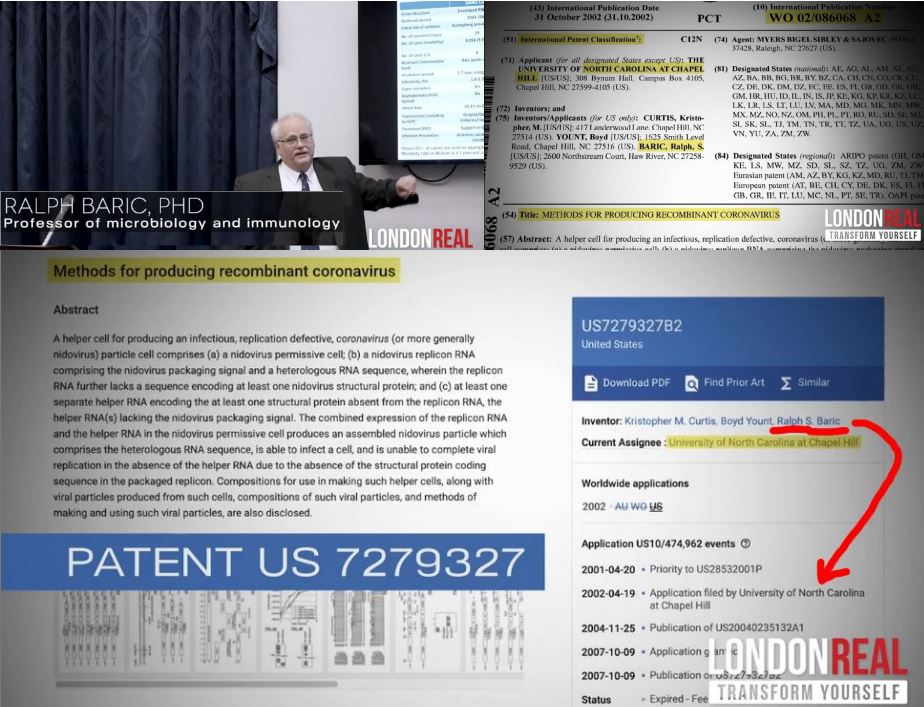
For instance, Professor Baric was among three inventors who patented techniques for producing a recombinant coronavirus, after filing for a patent on their work on April 19th 2002. This patent described the creation of helper RNA cells, which allegedly made the replicon RNA infectious because it was said to be able to complete viral replication with a structural protein coding sequence. This patent application was filed seven months before the first ‘SARS-COV epidemic’ emerged in November 2002.xi
According to Dr David E. Martin — whose company M-CAM tracks patent breaches of treaties, laws and ethics — Dr Fauci and his team of scientists had partnered with a team of Chinese scientists to study bat coronaviruses and their effects on human cells after the first SARS outbreak in late 2002.
In the school night length-documentary, Plandemic InDoctorNation, by Mikki Willis, Dr Martin said the World Health Organization was captured by a ‘Global Health Syndicate’. Dr Martin traced the patents on the coronavirus since 2002 — and believes that life insurers are the dominant group among the Covid Pirates, Privateers and Orchestra. In a recent lecture, Dr Martin pointed out that the mass killing of the elderly under the cover of a pandemic serves to save life insurers from huge payouts on policies by shortening their lives.
Therefore, while Daszak, Fauci and Baric were at the epicenter of research to alter the coronavirus, the world was being gaslighted to believe that only a natural origin narrative was plausible.
And for its part, The Lancet — which was founded in 1823 by English surgeon, Thomas Wakley, and was acquired in 1991 by one of the big six owners of science journals, Elsevier — participated in advancing this natural origin narrative. This publication of what amounted to psychological projection in the absence of rigorous openly available evidence, occurred on the watch of Richard Horton, who had been The Lancet’s editor-in-chief for a quarter of a century.
Dr. Richard Ebright, who is a board of governors professor of chemistry and chemical biology at Rutgers University, told Vanity Fair that only three labs in the world, at Chapel Hill, North Carolina, and at Galveston, Texas, and the Wuhan Institute of Virology were doing so-called gain-of-function research into the bat-coronavirus.
Ebright compared Daszak’s model of research — collecting samples from caves and mine shafts and introducing them to laboratories in urban environments, then sequencing viruses, growing cultures and producing more virulent genetically engineered strains — to “looking for a gas leak with a lighted match.”
The U.S. Centers for Disease Control and Prevention (CDC) evidently came to control the money flow from the patents on the corona virus, the disease, the detection and all of the measures, Dr Martin told documentary-maker Mikki Willis in Plandemic – InDoctorNation.
Crucially, in 2015, at a ‘workshop’ – “Rapid Medical Countermeasure Response to Infectious Diseases” – Dr Daszak talked about how the media hype in the next ‘disease outbreak’ could be used to convince the public of the need for a pan-global vaccine. Such media hype, Daszak added, would create the market that would attract investors to fund the mass development of vaccines, as the favoured medical countermeasure (MCM). At the time, Daszak’s EcoHealth Alliance – had become the funding conduit for ‘gain of function’ research for biological pathogens between Dr Anthony Fauci’s NAIID and the Wuhan Institute of Virology, China’s first level 4 biological military lab, as well as EcoHealth Alliance was also awarded $13.17 million from the Department of Health and Human Services.
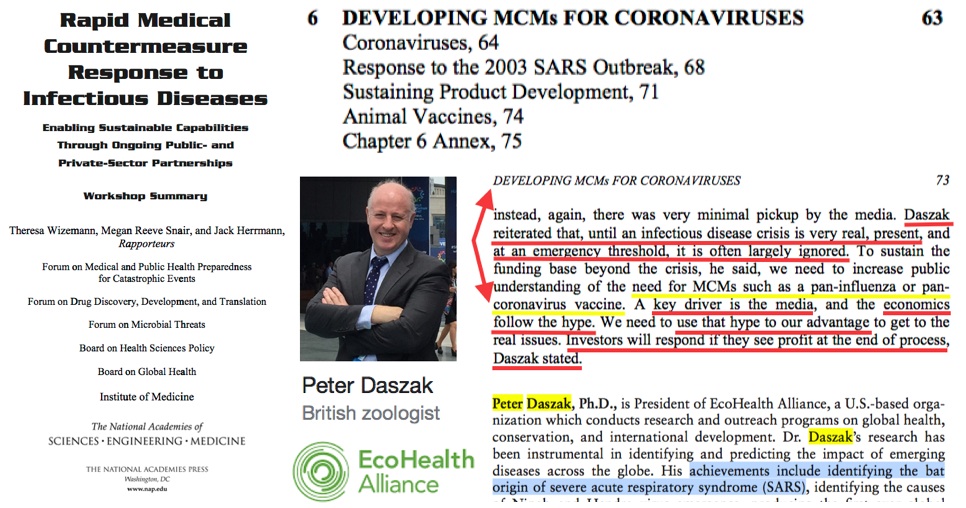
The subversive media hype idea suggested by EcoHealth Alliance Peter Daszak at the 2015 ‘workshop’ – “Rapid Medical Countermeasure Response to Infectious Diseases” – clearly penetrated the Global Health Security ‘community’.
Daszak’s subversive penetration ritual became a ‘flood the zone’ media strategy three years later at the UN’s first global pandemic exercise, Event 201, which took place in New York one month before the coronavirus outbreak was attributed to Wuhan City. Event 201 involved a natural outbreak of a species jumping, jet-setting zoonotic bat-pig coronavirus.
The central irony was that simulated newscasts were played at Event 201 that prepared participants to shut-down whole economies.
Meanwhile, the Pandemic Emergency Board discussed the need to get vaccine stockpiles, supply chains and other medical infrastructure financed, built and pandemic ready to mitigate economic mayhem!

Yet, the Event 201 tabletop exercise attributed blame for financial market crashes, widespread business failures and mass unemployment, to the coronavirus pandemic called Coronavirus Associated Pulmonary Syndrome (CAPS).
While this pandemic exercise was acknowledged in the public media after the onset of Covid-19 – and often with disparaging headlines about conspiracy theories – news reportage omitted the fact that Event 201 was the U.N.’s first global pandemic exercise.
Indeed, among the many omissions of key evidence in the pandemic rhetoric of Tedros Adhanom Ghebreyesus, WHO’s Director-General, the most glaring one is a ‘failure’ to mention the U.N.’s directive for a global pandemic exercise simulating the deliberate release of a lethal respiratory pathogen – before September 2020.
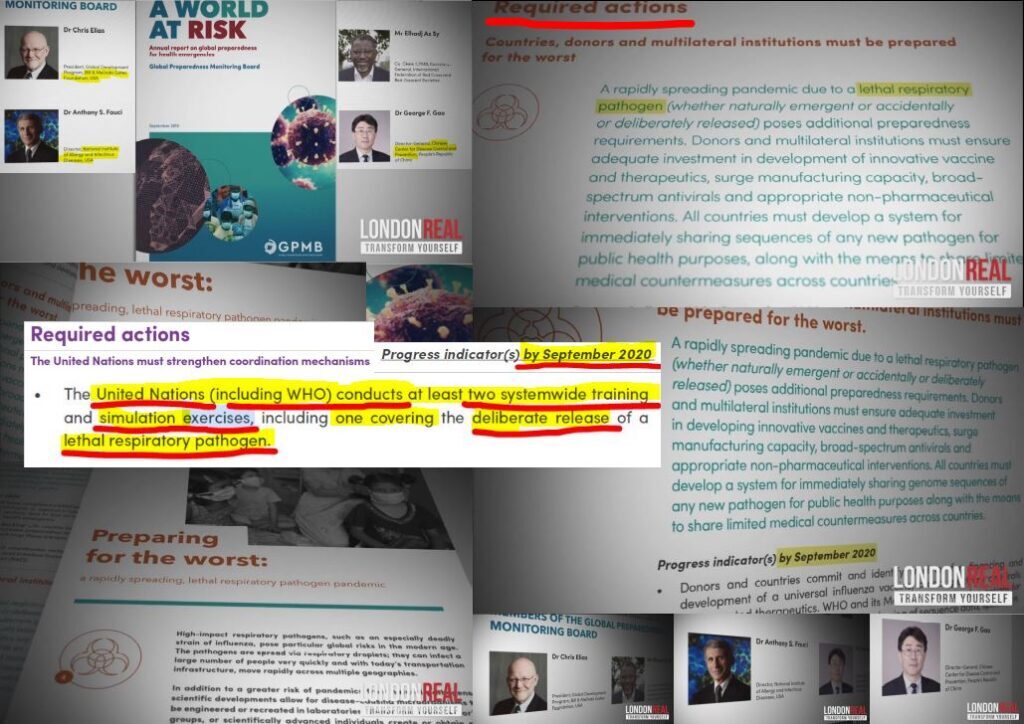
This omission is crucial, because if the world’s public had become widely aware that the U.N. had issued a directive for a global pandemic exercise, and it had taken place prior to Covid-19 – the narrative about a lack of preparedness would have become shaky.
Since, the Event 201 pandemic simulation could not be counted as a pandemic exercise involving the deliberate release of a lethal respiratory pathogen — and since Dr Daszak secretly organized 26 other scientists to sign off the natural origin narrative in The Lancet, which effectively mimicked the Event 201 script, it seems reasonable to wonder out loud if the WHO’s Covid-19 pandemic was an experimental exercise taken ‘live’.
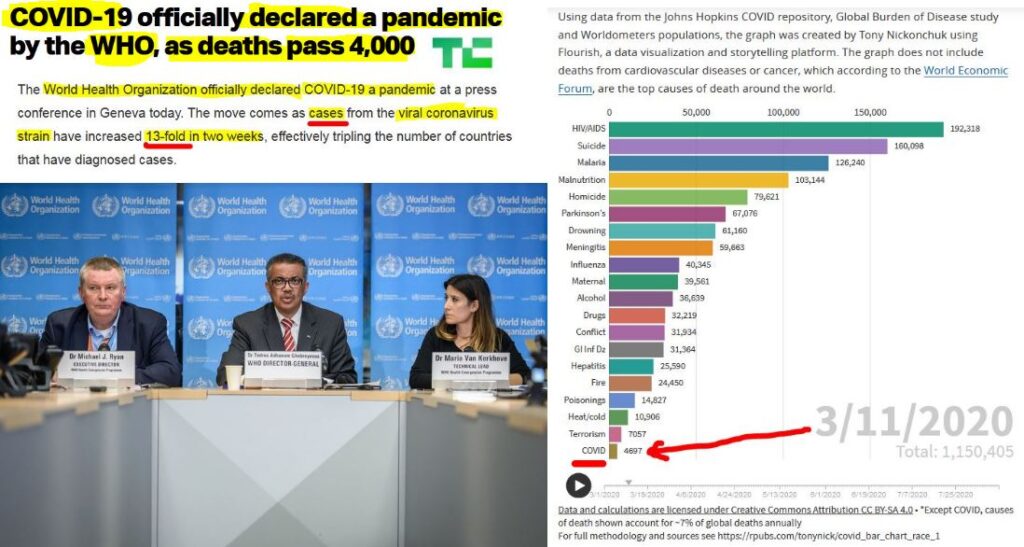
Especially since the global Covid-19 death toll was under 5000 humans at the time the U.N.’s World Health Organization declared Covid-19 a global pandemic.
How did the WHO decide Covid-19 was a global pandemic, when the threshold of 5000 deaths would barely register as an influenza epidemic in the world’s most populous nations such as China, India, Indonesia, Brazil, Russia or the United States of America?
Like The New England Journal of Medicine, The Lancet’s embroilment in publishing the statement — which was backed by early papers, including one from Ralph Baric — to quash such counter-factuals on the origins of the alleged SARS-CoV-2 coronavirus outbreak — has the hallmarks of colluding players advancing a game of medical democide.
By doing so, The Lancet helped foreclose investigation in an alleged viral outbreak that would be used to justify the imposition of medial martial law measures around the world, with devastating economic impacts that weaken the autonomy of households, the food security of whole nations and the health of the sick — as well as the healthy. The Lancet’s embroilment in legitimizing a single narrative also assisted in affording key individuals, institutions and interests the ideological room to make their next chess moves — without the worry of damaging defections.
In other words, The Lancet’s support at this time — 22 days before the WHO declared Covid-19 a global pandemic — was critical, because it cemented the natural origin narrative. This timing was crucial to the Corona Bandits, since they were forging a new hegemonic block necessary to gain buy-in from the mass publics for the construction of their desired solutions. If the most of the citizens across the UN system of nations came to believe that the alleged coronavirus outbreak was possibly the result of a lab-breach — let alone a bio-terrorist plot — the Corona Bandits’ desired solutions would have faced major skepticism, and therefore, tough obstacles.
The Corona Bandits’ desired solutions included: behavioural modifications such as anti-social distancing, bandit mask-wearing, and tyrannical house arrests (or medical martial law lockdowns); re-establishing misplaced trust in Big Government, Big Media and Big Pharma; and creating a global vaccine market, which would be linked to jurisdiction-based biomedical data systems, QR-code systems, and vaccine passport systems — that would become the basis for a global bio-security system.
However, the Covid natural origin propaganda would wear thin if the problem of sustaining a high enough death toll was not remedied once the initial death spike — following the WHO’s pandemic declaration — dropped off. If America’s newly-swelled news audiences saw the death toll plummeting toward zero in the United States before the Covid-19 vaccines could be brought to market, the entire Covid Psyop would have crashed too.
Enter the alleged anti-viral medicine, remdesivir, also known as Veklury.
The emergency use authorization of remdesivir, was made on the watch Commissioner Food and Drugs Administration (FDA) Dr. Stephen M. Hahn (2019-2021); director of the National Institutes of Health in Bethesda, Maryland, Dr Francis Sellers Collins (2009-2021), who is is an American physician-geneticist who discovered the genes associated with a number of diseases; CDC director Dr. Robert Redfield (2018-2021) and Secretary of the US Department of Health and Human Services Alex Michael Azar II (2018 to 2021), who was formerly head of pharmaceutical giant Eli Lilly’s U.S. operations.
Dr Redfield’s replacement at the US CDC, Dr Rochelle P. Walensky, who was formerly Chief of the Division of Infectious Diseases at Massachusetts General Hospital from 2017-2020, is also culpable. The Centers for Disease Control and Prevention (CDC) is legally bound to monitor the safety and effectiveness of medicines once they have been marketed.
In spite of these officials’ widespread expertise and experience, we are being asked to believe that widespread shutdowns of hospitals — except patients in critical care — as well as doctors’ clinics in numerous states, could not have been predicted to cause the death spikes — as detected by Dr Denis Rancourt in the All Cause Mortality statistics.
To fail to foresee such predictable consequences lacks plausibility.
Together, these Corona Bandits have played key roles in either engineering the Great Corona Planpanic, and/or authorizing measures to inflict medical democide, including the endorsement, authorizaton or approval of remdesivir, or for failing to recall Veklury (or remdesivir) when the so-called anti-viral drug was linked to multiple-organ failure, including impairing kidney function.
The Corona Bandits’ intention was to inflict democide.
➼ Step 3: Re-purpose the Drug from the Trial Run for the Live Global Simulation
The product description for Gilead’s Veklury — which is the brand name for the drug remdesivir — says its formulation claims to be a SARS-CoV-2 nucleotide analog RNA polymerase inhibitor (according to the Gilead’s product description, dated 10 October 2020, and submitted to John Farley, the FDA’s director of the Office of Infectious Diseases (OID).xvi
In other words, the drug remdesivir — which had been pulled halfway through the Ebola drug trial in 2018 — was re-purposed.
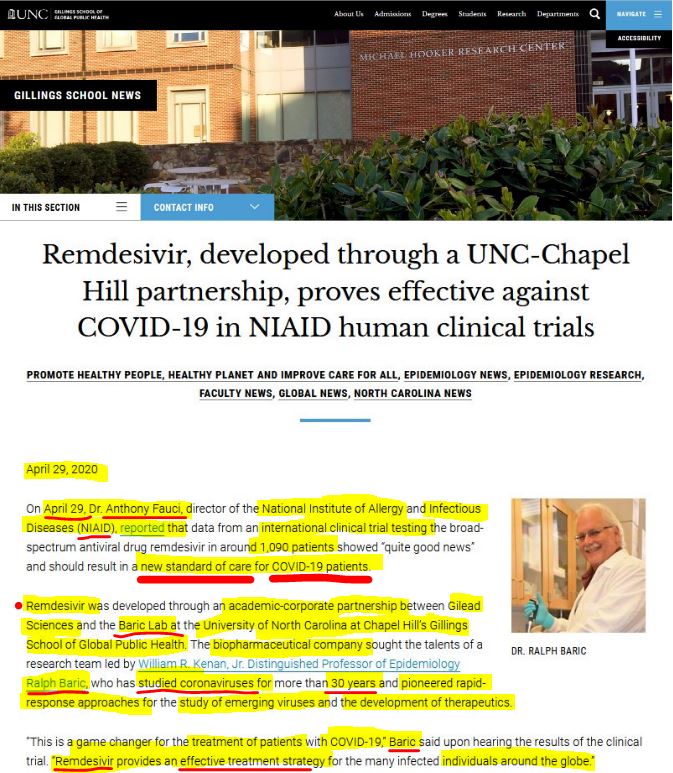
Remdesivir was developed by Professor Ralph S. Baric of the University of North Carolina at Chapel Hill campus, who as a long-time collaborator with Dr Anthony Fauci, studied the coronavirus for three decades, as the University of North Carolina bragged the same day that the NIAID director endorsed remdesivir from the White House.x
The drug was evidently re-designed in a partnership between Ralph Baric’s lab at the University of North Carolina and Gilead.xvii
Furthermore, Ralph Baric is one of the key players in a cohort of scientists who weaponized the coronavirus to make it pathogenic to humans over the two decade period leading up to the so-called ‘Covid-19 Pandemic’, says Dr David E. Martin.
It would appear, then, that the December 2019 paper in the The New England Journal of Medicine — which presented Remdesivir as the most lethal of the four drugs trialled on Ebola — created a problem that required a new study to fix the data with more favorable results.
Gilead’s next move was to sponsor a study that would be published in The New England Journal of Medicine on April 10 2020. The study, entitled Compassionate Use of Remdesivir for Patients with Severe Covid-19,v claimed the drug was effective at reducing patient recovery time.vi
Yet, 13% of vulnerable people died after completion of the treatment.
The cruelty of Gilead’s drug was also revealed in the adverse events metadata, because 60% of patients suffered adverse events, while 32% suffered serious adverse events, including: acute kidney and lung failure, or multiple organ failure, as well as septic shock and hypertension. Four were said to have ‘discontinued’ the trial because they required kidney transplants, which indicates they were pulled from the trial – lest they died from further ‘treatment’.
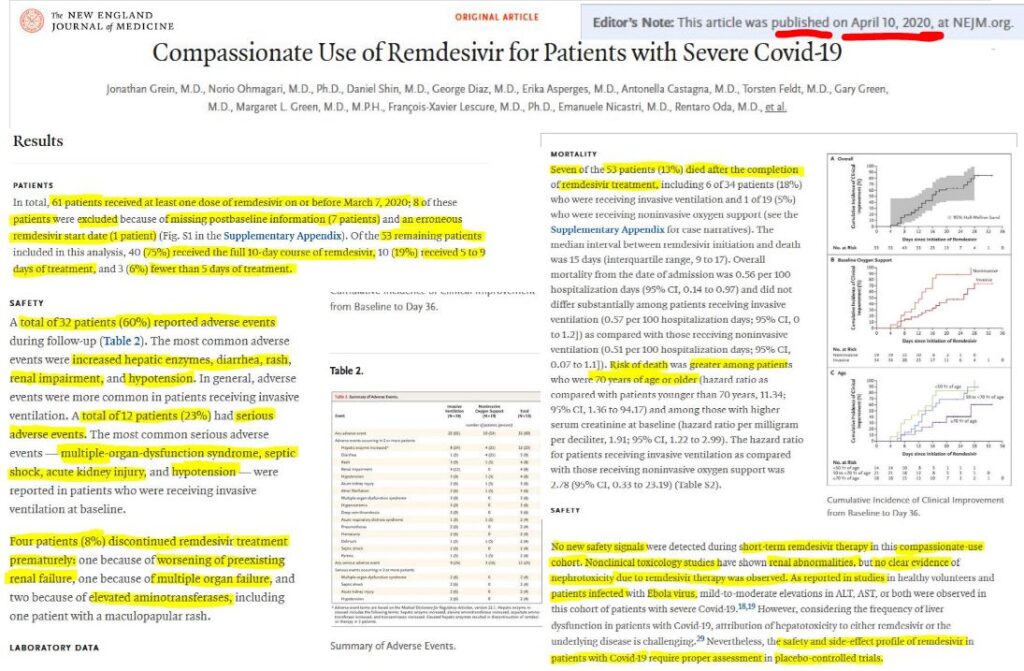
Moreover, this Gilead sponsored trial excluded patients with stage 4 Chronic Kidney Disease (CKD) and those receiving dialysis. Futhermore, Gilead’s Remdesivir trial lacked a proper control group, because it’s so-called placebo group also received the trial drug. This trashing of the scientific method was perpetrated to fix the trial data to achieve a more favorable result for citation, claims Dr Ardis in an interview with Ryan Cristian of The Last American Vagabond.viii
With these two studies — the 2018 Ebola four-drug trial and Gilead’s Remdesivir-Covid-19 trial — the sinister direction that the Covid Cartel was headed was signalled to those insiders attuned to such chess moves.
The NIH’s next move with Gilead — and in collaboration with The New England Journal of Medicine — was to begin recruitment on February 21 2019 for a 28-day Remdesivir trial with 53 Covid-19 patients.
This Remdesivir trial, known as the ACTT-1 Clinical Trial, was conducted at 60 trials sites, including: the United States (45 sites), Denmark (8), the United Kingdom (5), Greece (4), Germany (3), Korea (2), Mexico (2), Spain (2), Japan (1), and Singapore (1), with the first enrollments starting on February 21, 2020.
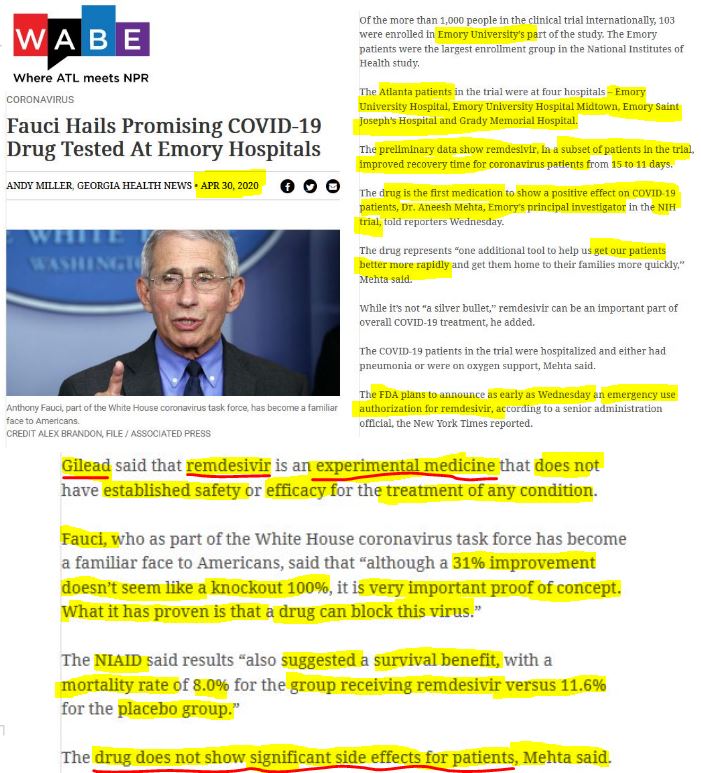
Four Emory University hospitals in Atlanta, Georgia, were involved in this trial, which was primarily funded by the Fauci-controlled National Institute of Allergy and Infectious Diseases. The drug, Remdesivir, was supplied by Gilead.
This new Remdesivir study, entitled — “Remdesivir for the Treatment of Covid-19 — Final Report” — published on October 8 2020, was deemed a success because the drug treatment shortened medium-term recovery time by five days, or 31% faster than the placebo group, and lowered respiratory tract infection.xii
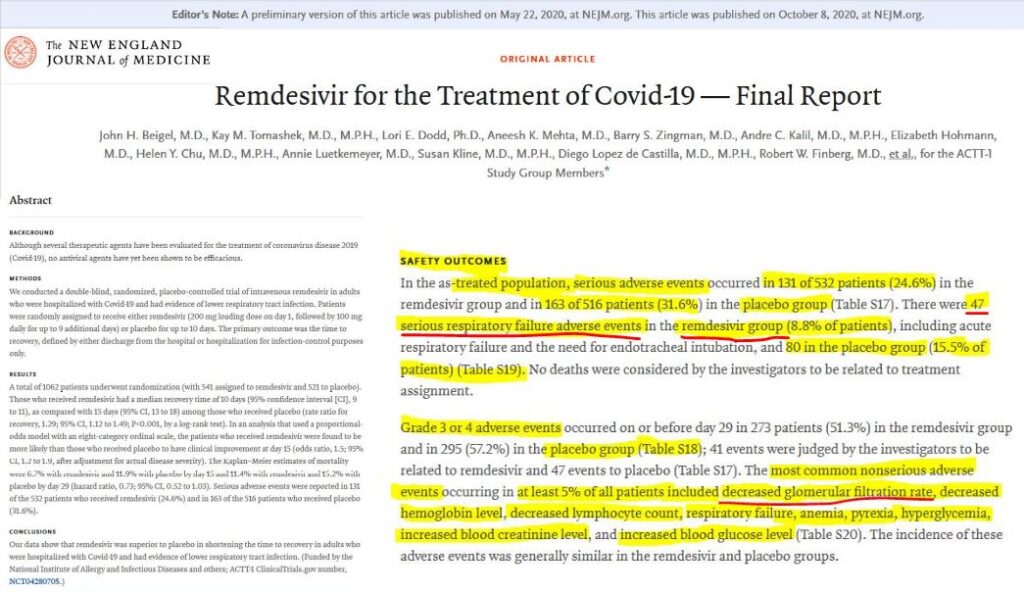
However, the upbeat conclusion of this new New England Journal Medicine study, which was initially published as a preliminary report on May 22 2020, was misleading because there was only a marginal improvement in reporting of serious adverse events between the groups. Serious adverse events accounted for 24.6% or 131 of 532 patients in the remdesivir group, and 31.6% or 163 of 516 patients in the placebo group.
Moreover, the Duke University School of Medicine’s Duke Antimicrobial Stewardship Outreach Network (DASON) the majority of patients in the study were on dialysis. Because a typical four hour intermittent dialysis session removes half of accumulated SBECD, this National Institute of Allergy and Infectious Diseases (NIAID)-sponsored study was not able to comment on patients with severe renal impairment who are not yet on dialysis.

Emory University’s principal investigator in this trial, Dr. Aneesh Mehta, told journalists on April 29, 2020 that Remedsivir was the first medication to show a positive effect on COVID-19 patients, reported WABE, an Atlanta public radio station.
Countering this viewpoint, Dr Ardis told Mike Adams of the Health Ranger Report that Dr Fauci set up a bogus trial to damage the standing of Hydroxychloroquine by setting the dosages at 10 times the proven standard, to cause heart failure and death through overdosing.xiv
Radio WABE reported that Dr Mehta claimed remdesivir does not show significant side effects for patients.
But, this new New England Journal Medicine study reported there were 8.8% of patients who suffered respiratory failure adverse events in the Remdesivir Group. The “Remdesivir for the Treatment of Covid-19” study also found a decreased glomerular filtration rate, which is a measure of the kidneys’ performance to remove waste water as urine.
The new study published by the New England Journal Medicine also reported that the investigators did not consider any of the 81 deaths to be related to the treatment assignment.
This claim is difficult for a reader without a subscription to the New England Medical Journal to unpack, because the main body of the report did not state what portions of the 81 deaths belonged to the remdesivir or placebo group. (Editor’s Note: The breakdown of statistics may have been left to numerous tables that were excluded from the free online version available).
Once this trial was completed, Dr Anthony Fauci — who has been the Director of the National Institute of Allergy and Infectious Diseases (NIAID), since 1984 — claimed the drug would “be the standard of care”, in a White House presser on April 29 2020.vii
By this statement, Dr Fauci appeared to preference controlling the metrics of dosage protocols to ensure that those who survived recovered 31% faster than those whom were chosen to die of known ‘side effects’, such as kidney failure, multiple organ failure and hypertension.
Fauci, who became a leading face of the White House coronavirus task force, said that “although a 31% improvement doesn’t seem like a knockout 100%, it is very important proof of concept. What it has proven is that a drug can block this virus.”
Twelve days prior, the National Institutes of Health published the findings of non-peer reviewed seven-day experiment using just 12 rhesus macaques monkeys alleged to have been infected with SARS-CoV-2 to test the performance of Remdesivir. The NIH’s media advisory claimed that the investigators found the data supported initiating remdesivir treatment in COVID-19 patients as early as possible to achieve maximum treatment effect.
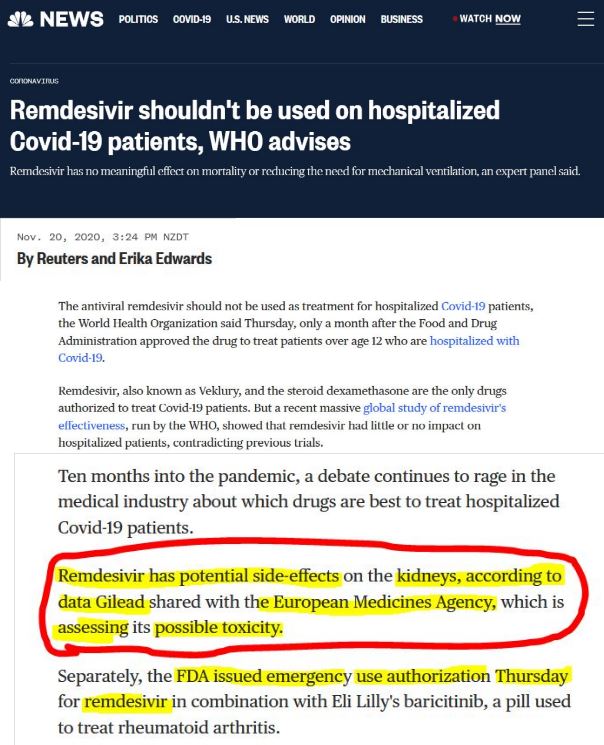
Then on October 5 2020, The Pharmalogical Journal noted that UK’s Drug Safety Research Unit (DSRU) were aware that the drug had been re-purposed from originally being developed to treat Ebola — in an article entitled, “EMA to investigate possible link between remdesivir and acute kidney injury”. Saad Shakir, director of the DSRU, said to The Pharmalogical Journal, that the paucity of safety data means we will need to keep reviewing and updating our benefit–risk analysis.
The European Medicines Agency’s Pharmacovigilance Risk Assessment Committee were set to investigate whether or not there was a causal relationship between Remdevisir and acute kidney failure.

Four days later, in an exclusive interview with the Gilead’s CEO, CNBC’s host of Squawk Box failed to question Daniel O’Day about whether, or not, the deaths of 8% of the patients that happened in the NIAID-funded international trial, occurred as a result of the drug under study.
Audaciously, O’Day claimed the trial was a ‘gold standard study’ because it had been peer-reviewed, and published in the New England Journal of Medicine the day before. CNBC’s lower third graphic straps talked up Remdesivir’s alleged benefits, claiming the drug significantly reduced viral replication, helped speed recovery and reduced deaths.

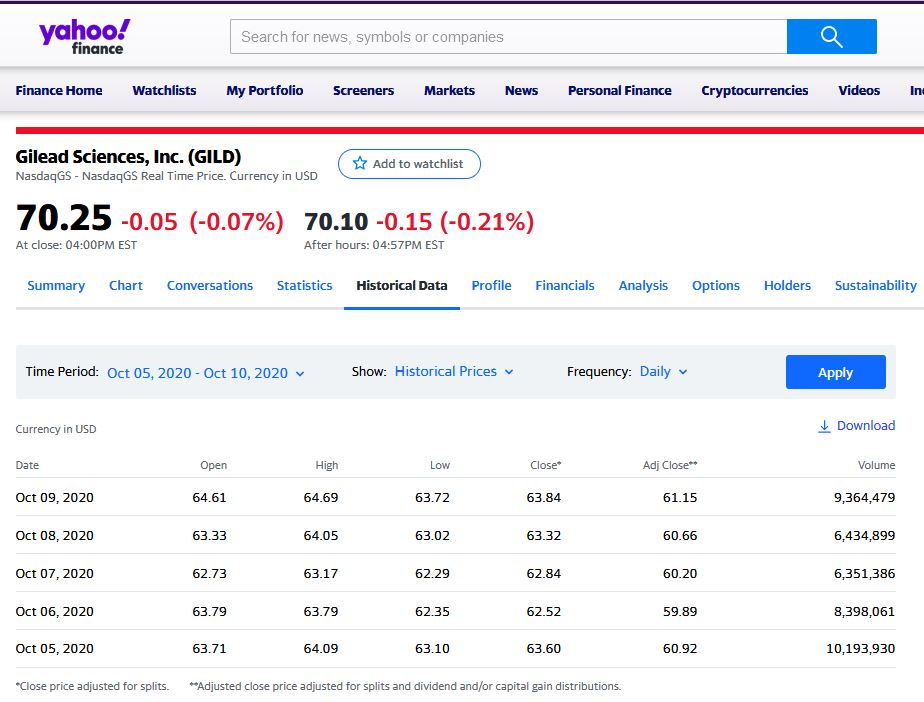
While O’Day spun Remdesivir’s value on the last financial market trading day for the week October 5 to 9 of 2020, CNBC supplied its audience was Gilead Sciences stock market value for the same week including real-time price values during the live on air interview.
Brazenly, one CNBC graphic that accompanied Gilead Sciences stock price graphic while O’Day was speaking on screen, read, “Gilead CEO: We will have sufficient global supply”. The subtext of the ‘exclusive interview’ was therefore coaxing CNBC’s viewers that now was a great time to buy shares in Gilead.
This Remdesivir trial was sponsored and primarily funded by the NIAID, National Institutes of Health (NIH), Bethesda, MD, and with additional funding from the the National Cancer Institute, NIH, and by the Department of Defense, Defense Health Program, and also by the governments of Denmark, Japan, Mexico, and Singapore. One of the trial sites in South Korea received funding from the Seoul National University Hospital. Support for the London International Coordinating Centre was also provided by the United Kingdom Medical Research Council.
Not surprisingly, the National Institutes Health doubled down on October 20 2020 in support of the Redemsivir study published in The New England Journal of Medicine. The NIH claim Remdesivir was “shown to be safe”, when the drug had been trialled in the Ebola outbreak, despite other investigational medications being deemed to have “worked better”.
It would appear the Remdesivir trial — which also included four Emory University Hospitals in Atlanta City — was designed to justify a poor performing drug that would actually cause many more deaths that could have otherwise been avoided if Ivermectin, Hydroxychloroquine and other therapeutics had have been used, as numerous doctors, scientists and nurses have said.xiii
And it would appear that these ‘trials’ were an experiment to figure out the relative lethality of the treatment dosages, rather than determine the drug’s safety and effectiveness to save lives.
After all, the US FDA issued an Emergency Use Authorization, just two days after Fauci’s endorsement of Gielad’s Remdesivir for the treatment of suspected or laboratory-confirmed Covid-19 in adults and children who were hospitalized with severe disease.
As the Director of the National Institute of Allergy and Infectious Diseases (NIAID), Dr Fauci set up a treatment protocol of one drug – Remdesivir – precisely because it was guaranteed to cause multiple organ failure in patients designated to have ‘contracted’ Covid-19, Dr Ardis claims.
Dr Ardis believes the intention behind this ‘make-shift’ drug protocol was to cause mass deaths, reproduce the mass fear generated at the beginning of the ‘pandemic’, and to justify the mass deployment of ‘vaccines’ by making Covid-19 appear more deadly than the data would otherwise show.
➼ Step 4: Supply Financial Incentives to Administer the Most Lethal Trial Drug
To incentivize hospitals to administer Remdesivir, the US Centers for Medicare and Medicaid Services (CMS) supplied codes to claim payments for the only drug authorized for Emergency Use by the FDA that became effective on 2 November 2020.
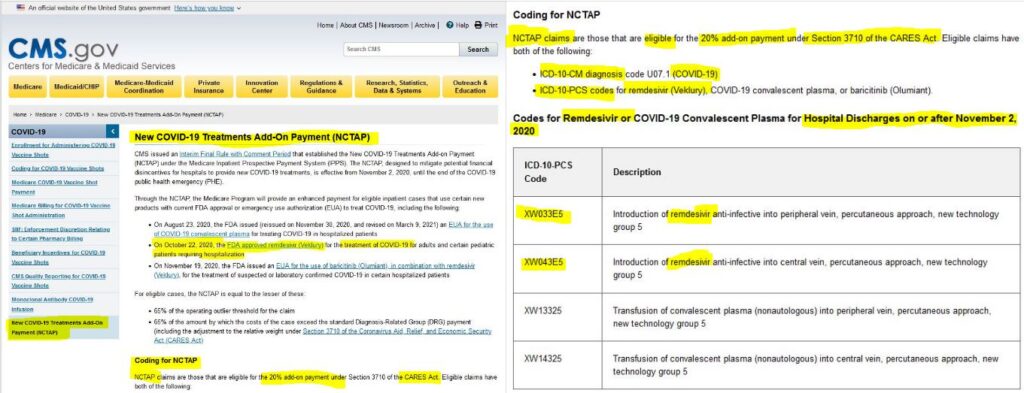
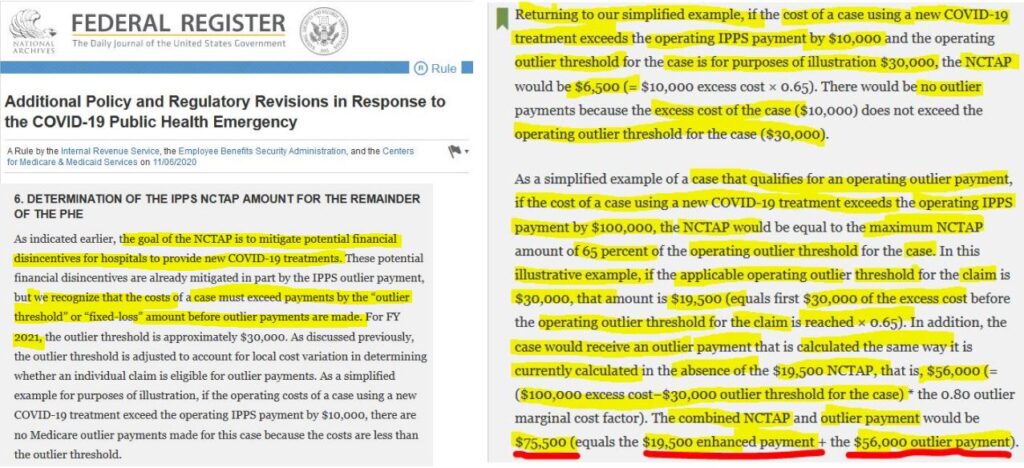
This financial incentives scheme became more formalized on the US federal Register on 6 November 2020 and laid out more comprehensive rules regime for claiming the new treatment costs for Covid-19 patients.xviii
This Medicare incentive scheme confirms Dr Scott Jensen’s disclosure of April 8 2020, that hospitals could receive $13,000 for a COVID-19 admission rather than usual Medicare claim of $3400 per patient.xix The hospital receives $39,000, if the patient goes on a ventilator for a period of at least 96 hours, according to a report produced by the Kaiser Family Foundation. This report noted that uninsured patients could still be billed for costs not met by the Medicare program.xx
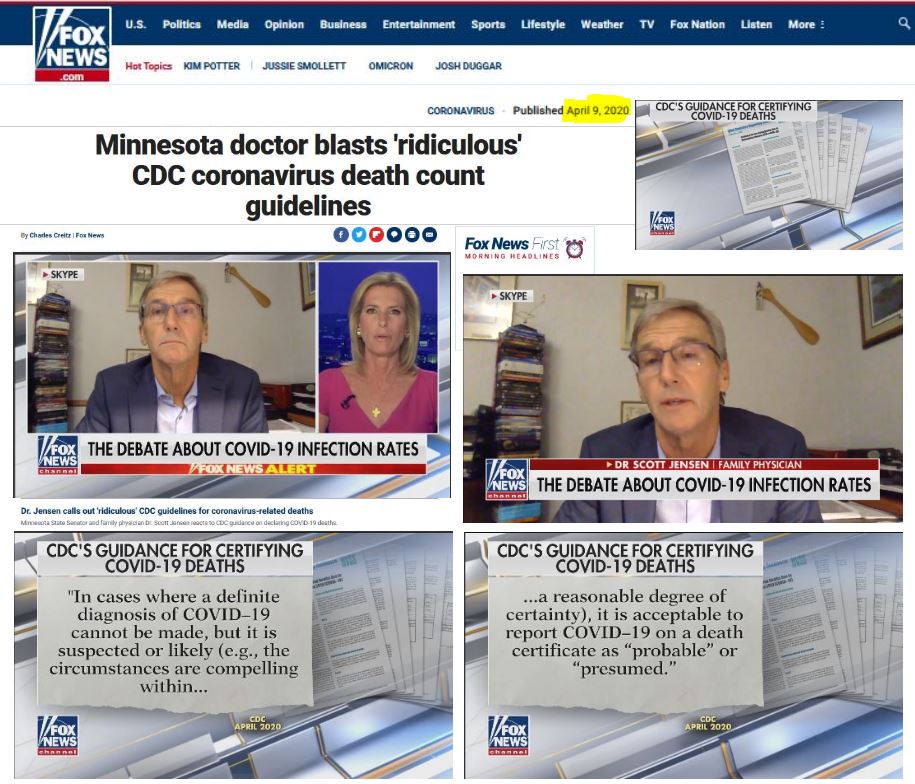
In an April 9 2020 interview with FoxNews, Dr Jenson, said he had received a seven page document from the CDC, entitled “Guidance for Certifying Deaths Due to Coronavirus Disease 2019 (COVID–19)”, instructing medical practitioners on how to fill out death certificates with a COVID-19 diagnosis. Dr Jensen pointed out that the CDC permitted doctors to report COVID–19 on a death certificate as “probable” or “presumed” in cases “where a definite diagnosis of COVID–19 cannot be made”.xxi
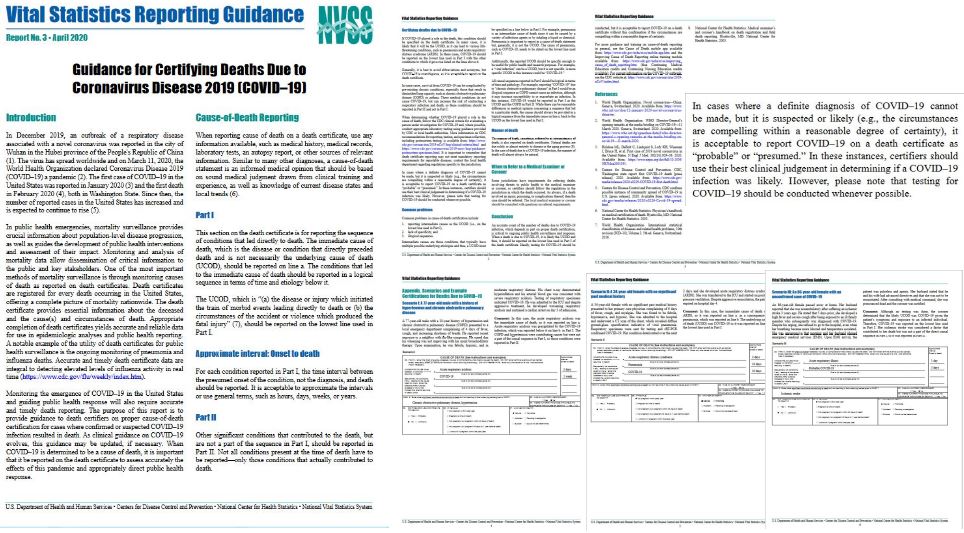
Dr Jensen, who at the time was a member in the Minnesota Senate, said that hospitals were being financially incentivized while the CDC was, in effect, coaching doctors to add Covid-19 on death certificates. Dr Jensen said such measures implemented amid an epidemic or a pandemic would lead to a gaming of the numbers and result in far-reaching impacts, including undermining public trust.xxii
Dr Jensen — like many earnest doctors who take the healthcare of their patients seriously — was unaware of the medical democide in the pipeline, while a number of studies sort to talk up Remedsivir, amid a systematic program of maligning the track record for existing therapeutics for treating viral infections.
➼ Step 5: Play Contrived Ignorance — Alphabet Health Agencies, Gilead & Fauci et al
The two early trials of Remdesivir for the Treatment of Covid-19 — which were both initially published by The New England Journal Medicine in April and May of 2020 — seemed to be geared toward justifying mass vaccine production of the final treatment solution to the alleged viral disease, Covid-19.
Because, Remdesivir was known to be lethal in the Ebola trial, and known to cause multiple organ failure, including kidney (renal) failure, which results in the body’s waste water flooding the lungs, causing pulmonary edema — key individuals, institutions and interlocked interests working to state-endorsed protocol are culpable for mass murder of targetted classes of humans, which meets the definition of democide.
By their repugnant enjoinable conduct, the perpetrators of this democide include: Dr Anthony Stephen Fauci as the Director of the U.S. National Institute of Allergy and Infectious Diseases (NIAID), Professor Ralph Baric at the University of North Carolina’s Gillings School of Public Health, the Executive Director of WHO’s Health Emergencies Programme, Dr Michael J. Ryan, and the Chairman and CEO of Gilead Sciences, Daniel O’Day.
Other culpable institutions include: the US National Institutes of Health (NIH), the University of North Carolina (Chapel Hill Campus), Atlanta’s Emory University, and The New England Journal Medicine, among others.
Some studies revealed a remarkable obtuseness to link the acute kidney injury and renal failure to Dr Fauci’s drug of choice, Remdesivir.xxiii
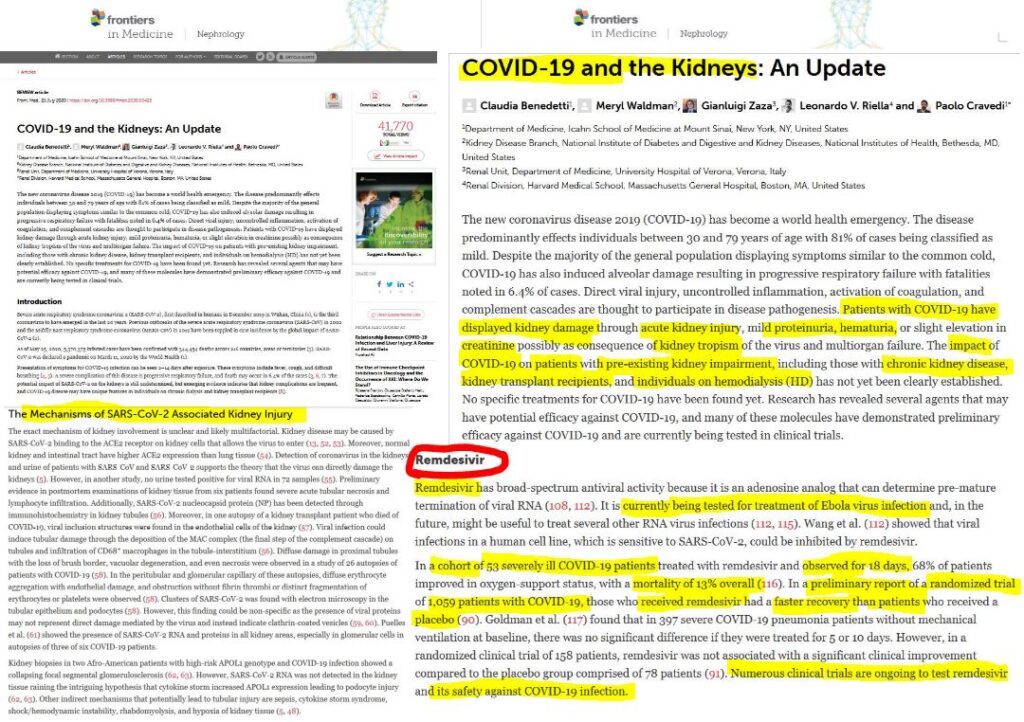
Strangely, the authors of an article published in Frontiers in Medicine, July 21 2020, mentioned remdesivir had been trialed to treat Ebola, but failed to cite the critical New England Journal Medicine study. This failure meant the doctors and scientists did not report that the mortality rate in the Remdesivir group was 53%.
In doing so, they let themselves off-the-hook to ask a critical research question: why was the most lethal drug of the four drugs in the Ebola drug trial preferenced by the FDA for emergency use to treat hospitalized Covid-19 patients?
Instead, they reported Gilead’s own rigged 53 patient trial, which had a mortality rate of 13%.
Had these research groups asked that critical question, they might have began to wonder if something was afoot.
Because— the pharmaceutical manufacturer of the least lethal drug in the Ebola drug trial had a new Vice President, Regulatory Affairs, seconded to Washington in August 2019, the same month that the NIH announced the Ebola Drug trial was to be foreshortened.
Regeneron Pharmaceuticals’s new VP, Dr Edward Cox, had jumped ship from his role as director of the Office of Infectious Diseases (OID) at the FDA.
On October 10 2020, Kidney International followed up with a study entitled, “Safety of Remdesivir with Acute Kidney Injury or CKD”, ostensibly to determine whether Remdesivir adversely impacted hospitalized Covid-19 patients with chronic kidney disease (CKD). The Kidney International study claimed most Covid-19 patients tolerated the infusion of Remdesivir well and asserted that no renal function abnormalities attributable to the drug were observed.
Yet, 30% of the patients — or 14 of the 46 Covid-19 cases whom were treated with Remdesivir — died.
Other study groups appeared to either question the US Alphabet Health Agencies claims, check the performance of Remdesivir in the 2018 Ebola Trial, and listen to reports of kidney failures, before formulating study protocols to review the databases to check for adverse events connected to the drug.
In referring to one particular study of Covid-19 patients subjected to Remdesivir entitled, “Remdesivir and Acute Renal Failure: A Potential Safety Signal From Disproportionality Analysis of the WHO Safety Database”, and which was published on the NIH’s PubMed website,ix Dr Ardis said the research group proved what Dr Fauci and Dr Ryan already knew.

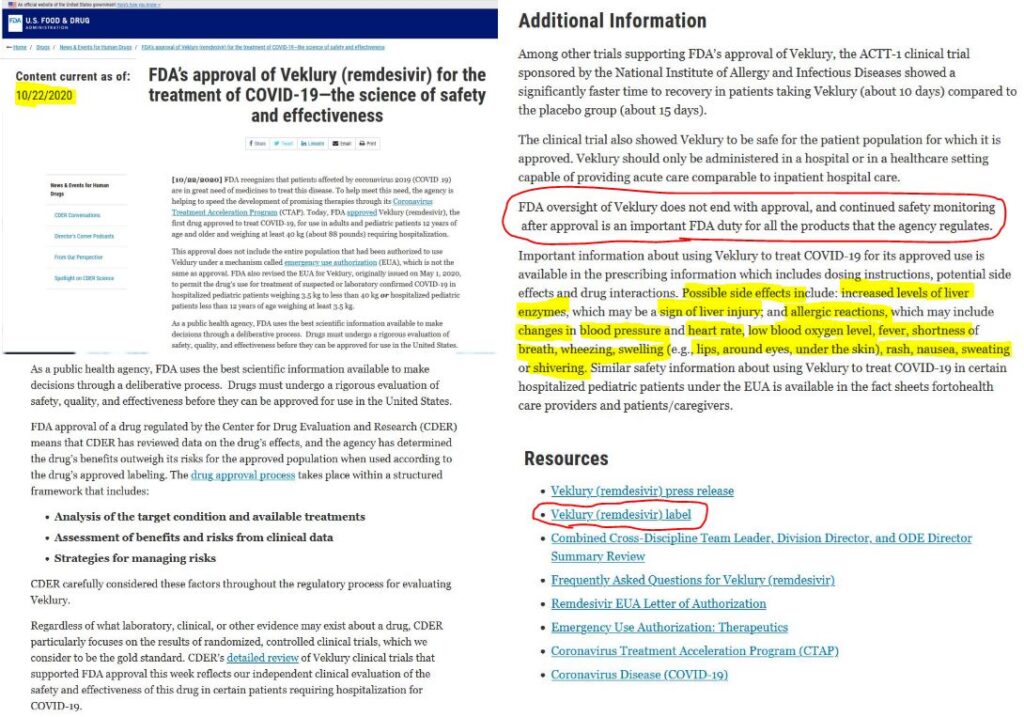
Ironically, on 22 October 2020, the US FDA issued Gilead’s product description sheet for VEKLURY, which warns of renal impairment and liver inflammation issues.
On October 22 2020, the US Food and Drug Administration cited the ACTT-1 clinical trial sponsored by the National Institute of Allergy and Infectious Diseases when the food and drug regulator granted approval for the use of Gilead’s Veklury brand of Remdesivir. The FDA webpage announcing this full approval neglected to mention that renal failure and acute kidney injury were at that time known to be ‘possible side effects’. Indeed, the known kidney-related side effects are briefly described in the Veklury package insert downloadable from the “Resources” at the bottom of the page.
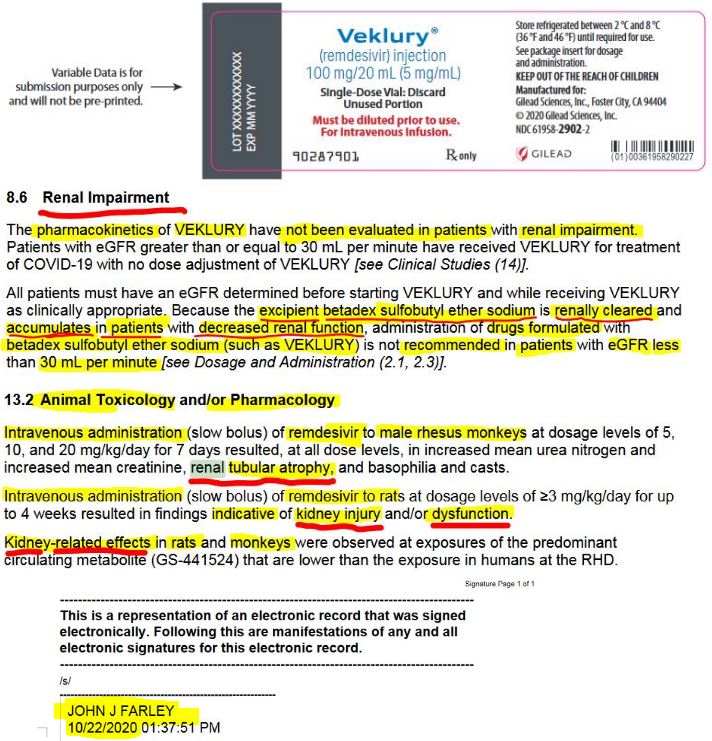
In the Full Prescribing Information submitted to the FDA, Gilead disclosed that Veklury’s expicient ingredient is betadex sulfoutyl ether sodium, which unhealthy kidneys cannot process effectively.
This problem of increasing impaired renal function causing reduced the solubilizing agent sulfobutylether-β-cyclodextrin (SBECD) clearance was reported on the US National Institute of Health website on 26 March 2018, in an article entitled, Clinical Pharmacokinetics of Sulfobutylether-β-Cyclodextrin in Patients With Varying Degrees of Renal Impairment.
This finding, which was published in the June 2018 edition of the Journal of Clinical Pharmacology, was five months prior to the decision of the NIH’s National Institute of Allergy and Infectious Diseases (NIAID) to sponsor the four drug trial that included Remdesivir to test drugs in the Ebola outbreak in the Congo Republic.
Gilead were well aware of the problem of sulfobutylether-β-cyclodextrin (SBECD) being associated with impaired renal function. The awareness is why Veklury’s product prescribing information ‘highlights’ warned that the product was not recommended for patients below a certain kidney filtration rate, termed as an estimated glomerular filtration rate measured in millilitres per minute.
In Gilead’s product label insert, severe renal impairment is measured at eGFR < 30 mL/min, or an estimated glomerular filtration rate of under 30 milliliters per minutes.
In November 2020, the World Health Organization, advised that Remdesivir (Veklury) not be used to treat hospitalized Covid-19 patients, just one month after the FDA approved its emergency use for hospitalized humans of 12 years old and older.
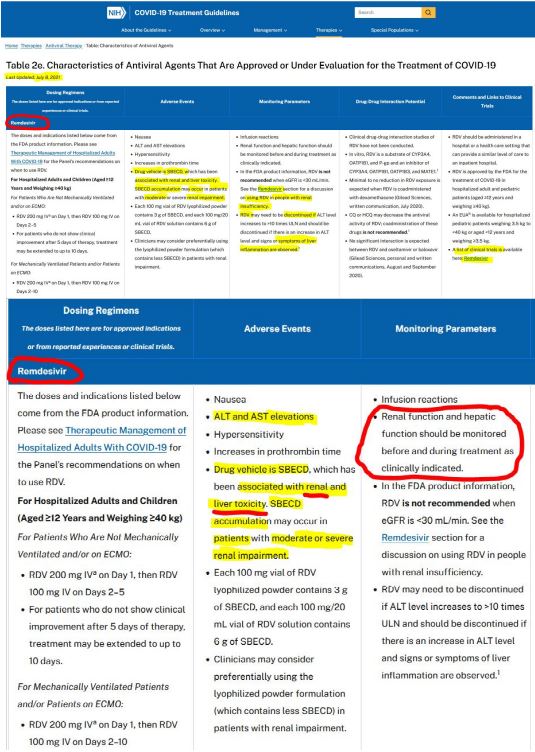
Ironically, the National Institutes of Health (NIH) website warns that Remdesivir is associated with renal and liver toxicity and the drug’s use should to be monitored to ensure that renal and liver function are not adversely impaired.xv
In the subsection, ‘Dosing Regimens’, the NIH notes that the ‘drug vehicle’ in Remdesivir is SBECD, and warns that the substance may accumulate in the kidneys in patients with moderate or severe renal impairment. The listed antiviral agents that were either approved or under evaluation as this July 8 2021 update shows.
These findings confirm what Dr Bryan Ardis has been warning America about since mid-June of 2020. Dr Ardis and other dissenting, doctors, nurses and scientists say the United Nations’ member governments are worsening the real emergency. For instance, a Covid Pandemic Panel of scientists and doctors stated in September 2021 at San Juan Puerto Rico this political interference involves the dismissal of known therapeutics, biasing mass deployment of poorly-tested harmful experimental nano-gene injections, and fostering a politicization of medicine, public health and personal health choices.
Dr Ardis says doctors working in American hospitals have became aware of his alarm calls, and have sought to get the hospital treatment protocols changed to discontinue the use of Remedesivir and switch to other therapeutics. But, hospital boards who have become authoritarian during the alleged ‘global Covid-19 pandemic’ refuse to allow the change, says Dr Ardis.
According the U.S. Department of Health and Human Services, a total of 650,000 treatment courses of Veklury (remdesivir) was made available to state and territorial health departments by HHS/ASPR from May 4 – September 30, 2020, for use in in U.S. hospitals to treat COVID-19 patients. On December 1 2021, Gilead announced Veklury and the generic anti-viral Remdesivir have been made available to more than nine million patients around the world, including 6.5 million people in 127 middle- and low-income countries through our voluntary licensing program. Gilead donated 450,000 doses to India, which is among the 50 countries that have approved or authorized Veklury for temporary use.
Therefore, this investigation supports the view of Dr Bryan Ardis that Gilead’s branded Remdesivir drug Veklury was used to mass murder vulnerable Americans from May 2020.
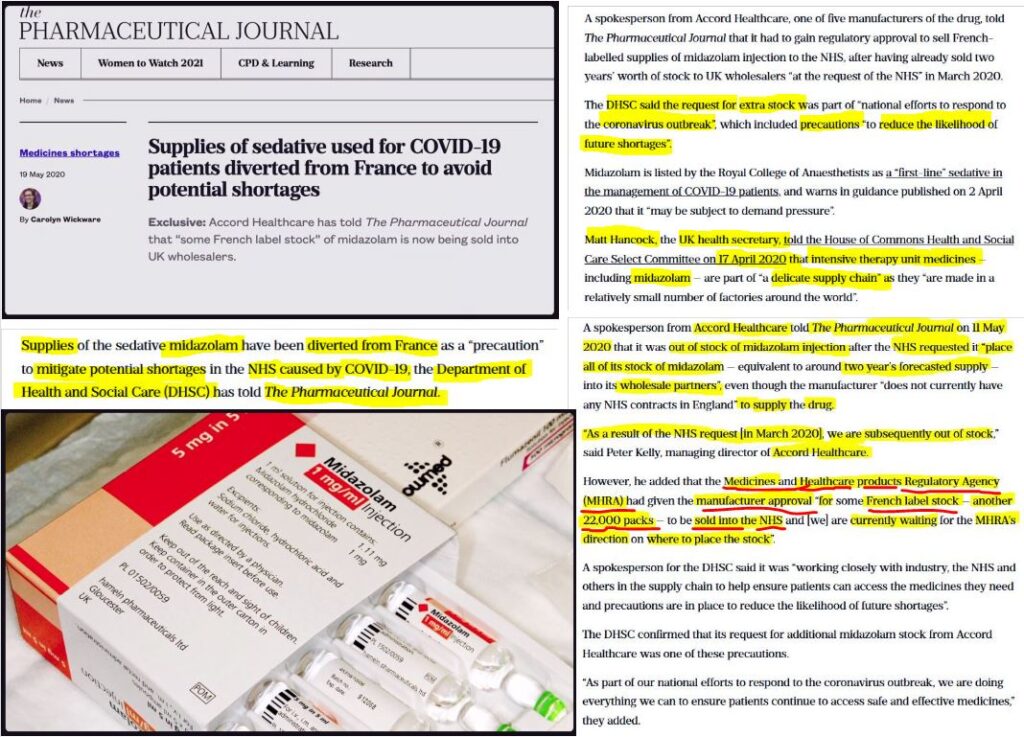
➼ The Midazolam Murders — Medical Democide in the United Kingdom
This view is supported by Stuart Wilkie in England, who has shown that the UK health authorities used a drug called Midazolam in combination with Morphine to kill the elderly of Britain from the beginning of the so-called global pandemic. Wilkie — who is featured in a documentary titled, A Good Death? — explains that both drugs are respiratory depressants and have a con-comitant effect that slows breathing with increasing dosages.
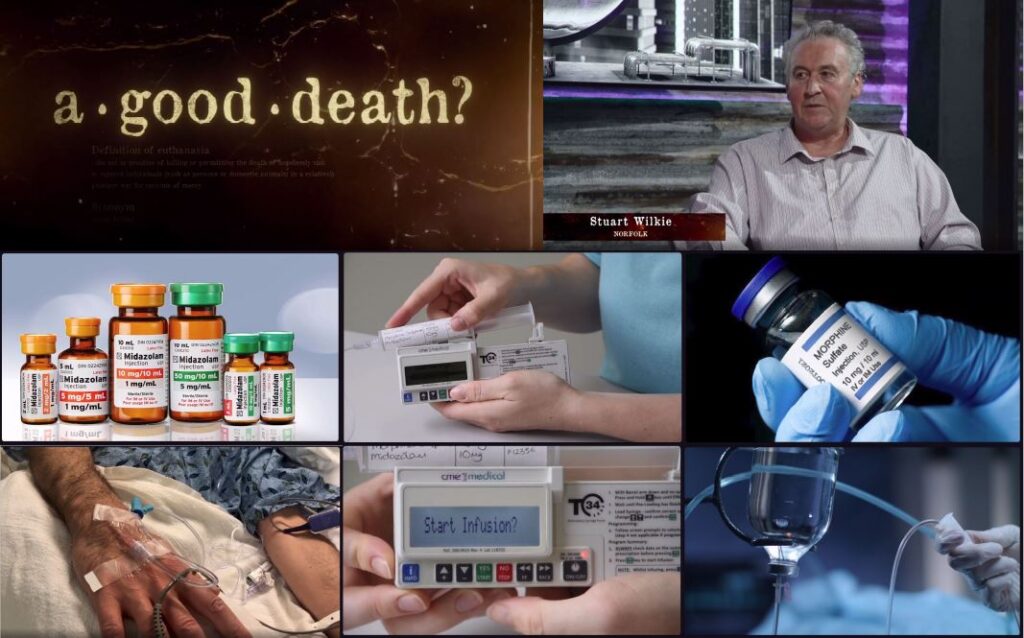
On May 19 2020, The Pharmaceutical Journal reported that the UK’s National Health System (NHS) had bought 22,000 packs of a sedative Midazolam from France. This stock order followed the NHS’s requisition of stock in March 2020 of Accord Healthcare’s 2-year supply, which had run out by end of April.
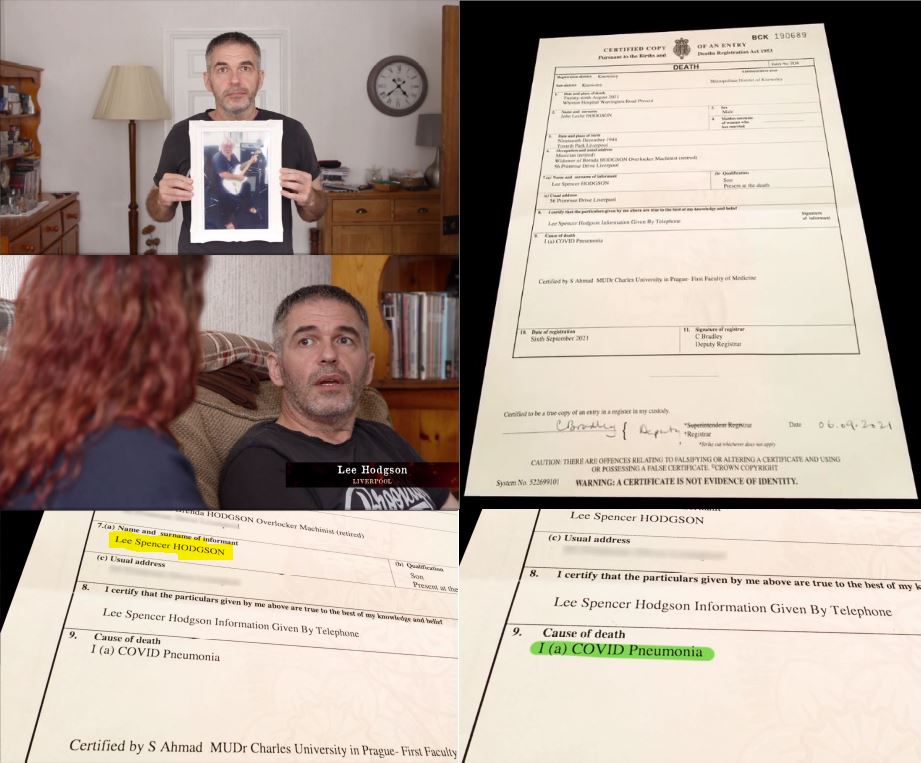
Among the hundreds of people that journalist Jacqui Deevoy interviewed for the documentary A Good Death?, Lee Hodgson’s ordeal with the NHS was tragically common. Hodgson believes his father was murdered as part of a program to boost the United Kingdom’s Covid death statistics. Hodgson said his father’s official cause of death was attributed to COVID Pneumonia, rather than the drug combination of Midazolam and Morphine.
Because the drugs suppress breathing, patients are unable to respire air and water vapor, causing a build-up of water vapor on the lungs. Hence, the symptoms of pneumonia were attributed to Covid, which is described as a highly transmissible coronavirus respiratory disease that mostly affects the elderly with co-morbidities.
Wilkie added that there is a paradoxial effect of drugs whose side effects, or stealthily intended effects, cause the symptoms that doctors use to claim patients are at ‘end of life’, and commence ‘palliative care’ to accelerate their demise.
This systemic program of medical democide occurring in the United Kingdom under the rubric of a global Covid-19 pandemic supports the argument of Dr Bryan Ardis, that the similar mass murder program was inflicted on unwitting patients in the United States by a stealthy transnational network of eugenicists.
But efficacy of this medical democide plot could not work if other effective therapeutics with proven track records were not sunk in the mass public consciousness in the United States, and around the Western world.
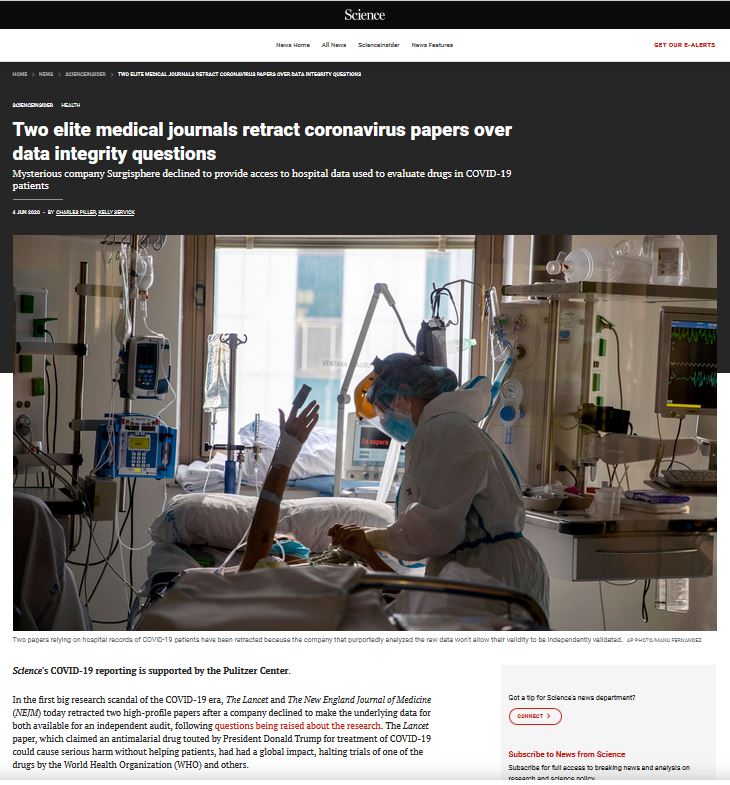
➼ Retractions by The Lancet and The New England Journal of Medicine
The use of Remdesivir as a novel anti-viral medicine relied in part on the narrative that the alleged disease, Covid-19, was caused by a novel coronavirus. In addition to the coronavirus patents awarded to Dr Ralph Baric, the CDC and other scientists for their alterations to the coronavirus, including the distinctive spike proteins that were subsequently used as the active ingredient in all Covid-19 bioweapons marketed as ‘vaccines’ — this supposed novelty in cause and remedy implied there were no existing effective therapeutic treatments.
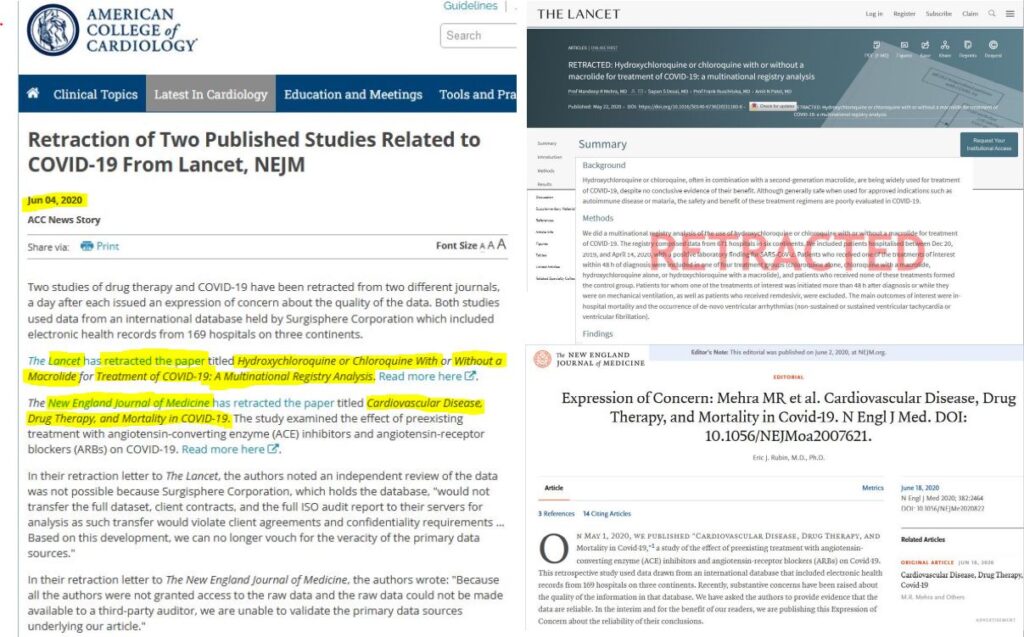
On May 22 2020, The Lancet, published a study numbingly titled: “Hydroxychloroquine or Chloroquine with or without a Macrolide for treatment of Covid-19: a multinational registry analysis” was based on a massive database, that had purported to find harmful effects associated with the antimalarial drug, hydroxychloroquine. But, the study swiftly drew flak from scientists about the veracity of the data, and about that database’s owner, Surgisphere Corporation, and its refusal to make its raw hospital patient database available for scientists to independently audit.
The New England Journal of Medicine also published an article based on data from the same database owned by Surgisphere, claiming that certain blood pressure drugs, including angiotensin-converting enzyme (ACE) inhibitors, didn’t appear to increase the risk of death among COVID-19 patients, as some researchers had suggested.
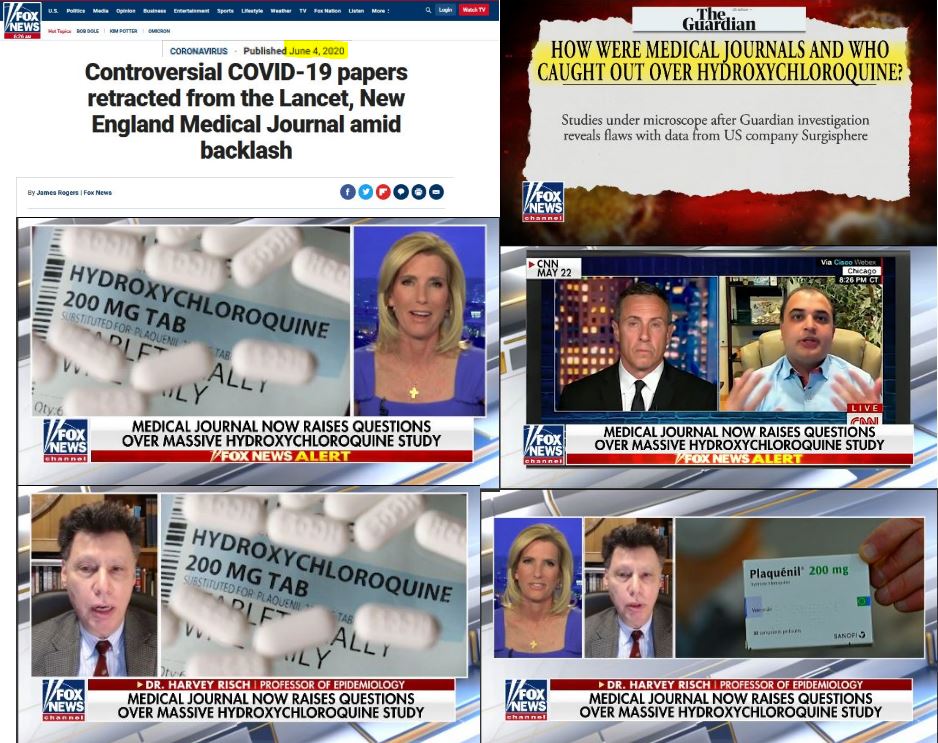
Just thirteen days later after the Lancet hydroxychloroquine was published, The Scientist magazine reported on June 4 the impacts of the studies published in The Lancet and The New England Journal of Medicine, upon news that both medical journals were forced to retract the papers. In an article headlined Lancet, NEJM Retract Surgisphere Studies on COVID-19 Patients, The Scientist wrote:
❝Surgisphere’s studies have contributed to shaping the global pandemic response. The World Health Organization and other health groups, for instance, had suspended testing of hydroxychloroquine in response to the Lancet paper, although the WHO has since reinstated the study.❞
The controversy escalated when The Guardian investigated the Surgisphere Corporation, which reported the science editor of the small Chicago-based company operated by Sapan Desai — the fourth author of the study — appears to have made the career move from science fiction author and fantasy artist. Meanwhile, another employe appeared to have re-invented herself as the company’s marketing executive after being an adult model and events hostess.
Adding to the intrigue behind the Surgisphere database, Dr. Jonathan Fishbein, President of Veracuity, a bio-pharmaceutical safety, informatics and analytics firm based in Pensylvannia said:
“How do you get so much data that quickly? It’s extremely difficult and time consuming to negotiate data sharing agreements with hospitals. That should have set off alarm bells. It would have been an issue to pursue before deciding to publish what seemed to be such a seminal paper.”
Despite, these retractions, the damage was done, and the efficacy of hydroxychloroquine and other therapeutics were sunk in the public mind, and it became a heresy across many Western countries of the U.N. system for hospitals, clinics and elderly care homes to prescribe therapeutics with a proven track record.
Therefore, to shore-up the medical fiction that Covid-19 required novel therapeutics for treatment of a novel strain of coronavirus, The Lancet enjoined itself in furtherance of the conspiracy to hoodwink the world that the anti-viral medicine, hydroxychloroquine, was ineffective at treating Covid-19 patients.
With this wedge tactic, The Lancet’s major contribution was to damage hydroxychloroquine’s reputation, short-circuit the World Health Organization’s sponsored trial of hydroxychloroquine as a Covid-19 treatment and to help thrust Gilead’s Veklury brand of Remdesivir onto the treatment protocol manifests of hospital boards across the United States.
➼ The New York Remdesivir Murders amid the Great American Corona Democide
These findings support the claims of Dr Bryan Ardis that America’s hospitals became (un)witting conduits for legitimizing mass murder of specific classes of vulnerable humans who were deemed as suspected or laboratory confirmed cases of an alleged lethal respiratory disease claimed to be novel, ‘SARS-COV-2‘.
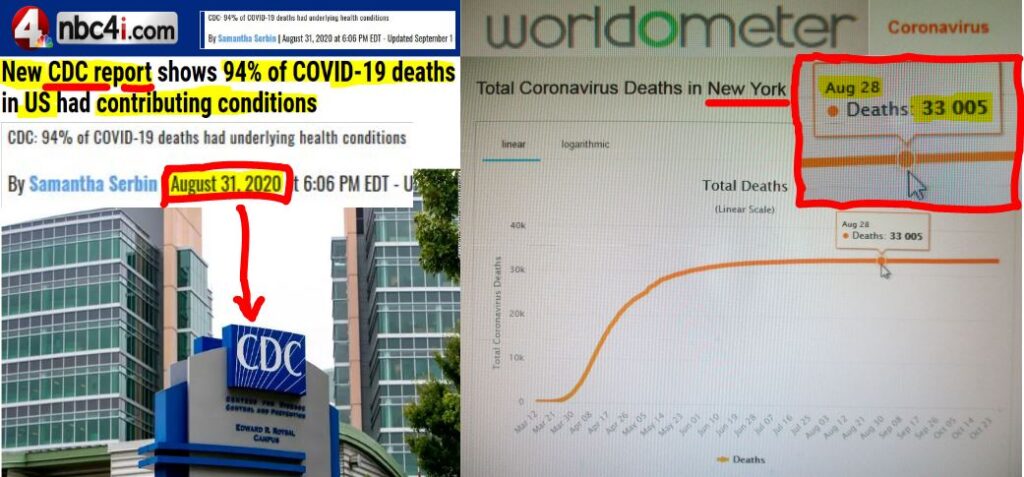
On the very last day of August 2020 – New York State reached a horrendous ‘milestone‘ death toll of 33,000 on Friday August 28th, which just happened to coincide precisely with the CDC’s report for the week ended August 29th.
Crucially, this was the CDC’s last report before an all important September 2020 cut-off date set by the U.N.’s Global Preparedness Monitoring Board (GPMB), for at least two global pandemic exercises to be conducted, across the United Nations system of member countries. The first exercise, called Event 201, which involved a natural outbreak of a species jumping, jet-setting zoonotic bat-pig coronavirus, occurred precisely one month after the U.N.’s GPMB), published its report — “A World at Risk” — on September 18th 2019.
It’s my contention that the ‘Covid-19 Pandemic’ was treated as a ‘live exercise’ by key conspiring players in the United Nations, including the World Health Organization, and the world’s major and significant states, including health departments, medical boards, hospitals and nursing homes.
In this repugnant game of medical democide, New York State — in essence — ‘won’ the gold medal in the 1st ‘Live’ United Nations’ Corona World Games for a State Territory within a Nation State Jurisdiction to reach the milestone Covid death toll of 33,000 first.
When New York State reached this milestone on Friday August 28th, the 33,000 death count just happened to coincide precisely with the CDC’s report for the week ended August 29th, and, therefore, just in time for the United Nations’ deadline (to complete at least two global pandemic exercise by September 2020). In effect, key New York State health and emergency, county and state, as well as hospital, nursing home and clinic officials – were boasting they had supreme control of the Covid-19 data out of all jurisdictions in the United States and were the most daring players in the United Nations’ Corona World Games.

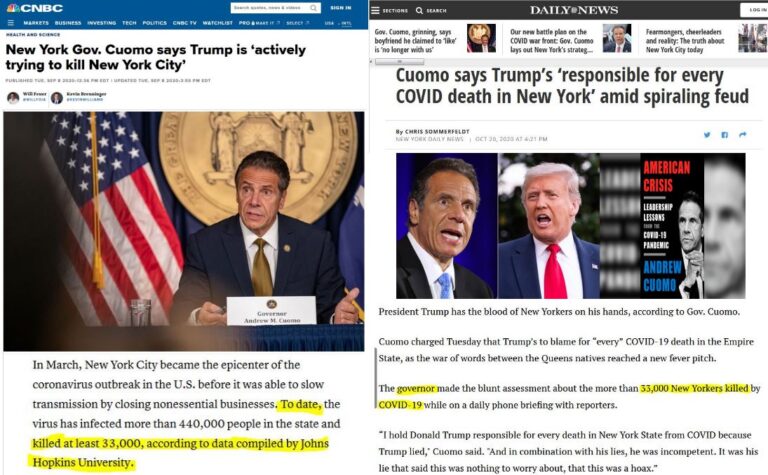
New York Democrat Governor Andrew Cuomo and Republican President Donald Trump played along by supplying political puppetry to make dramatic headlines. Cuomo asserted Trump was “actively trying to kill to New York City”. Trump spat back, and this feud continued into October. Meanwhile, the Establishment News Media continually mentioned the 33,000 milestone death count in the articles.
This control of data is crucial to bear in mind.
Because – when the U.S. Centers for Disease Control (CDC) published its Provisional COVID-19 Death Counts for the United States at this time (for the week-ended Saturday August 29 2020), the results showed that 94% of patients whom were counted as Covid deaths had other morbidities, or serious health conditions.
Given that Remdesivir did not gain emergency use authorization until May 1st 2020 in the United States, what could have accounted for initial deaths attributed to Covid-19, during the ‘1st wave’ and that peaked in April 2020?
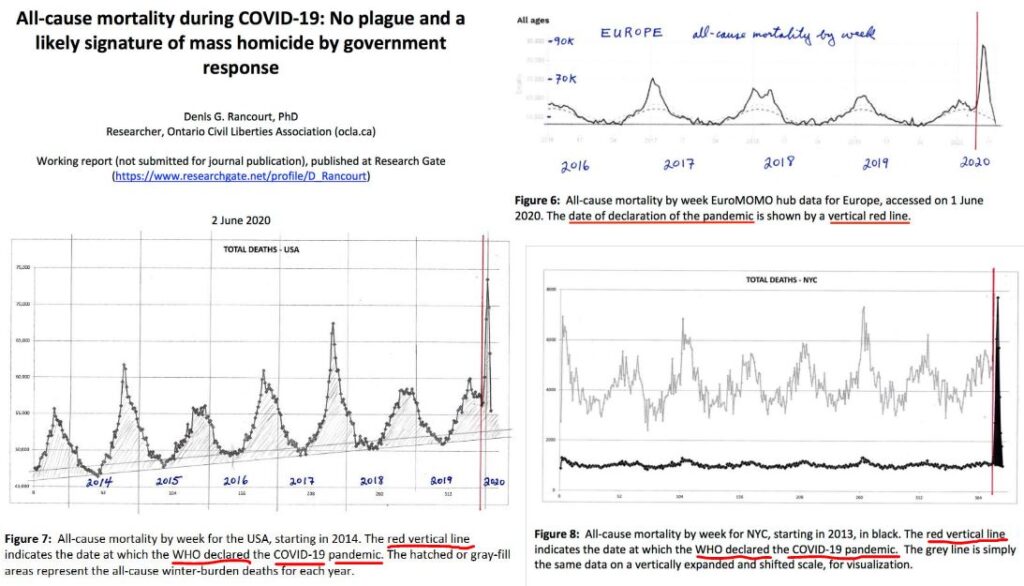
Striking peaks in deaths occurred in places where central, state or county governments had imposed draconian ‘pandemic’ measures immediately after the World Health Organization’s pandemic declaration of March 11 2020, as Dr Denis Rancourt discovered. The former professor of physics at the University of Ottawa, interrogated All Cause Mortality data, which measures the total number of deaths by place, time and demographic, across numerous jurisdictions.
In his paper “All-cause mortality during COVID-19: No plague and a likely signature of mass homicide by government response” published in June 2020, Dr Rancourt interrogated the All Cause Mortality data across multiple jurisdictions of Eurpope and North America. Dr Rancourt showed that the lockdowns triggered by WHO’s pandemic declaration of March 11 2020 resulted in clear death spikes in April and May of 2020.
Across numerous jurisdictions of the UN member state system, the disproportionate lockdown measures included the shutting down of hospital services for all but those in critical care, the curtailment of clinic visits and the widespread shutdown of economic activity.
For instance, Rancourt found there was a “COVID peak” in the USA data that arose from the first two months of state-wide lockdowns, across some states, where deaths were accelerated by human intervention, or those who were in poor health or convalescing, and had been thrust into more precarious and stressful living conditions. Rancourt showed that “hot spots”, such as New York City (NYC), had such Covid Peak spikes, whereas California did not have such an attenuated COVID Peak, during April and May of 2020, despite its lockdown.
Strikingly, Dr Rancourt also found that there was no “COVID peak” in any of the seven states that declined to impose a lockdown: Iowa, Nebraska, North Dakota, South Dakota, Utah, Wyoming, and Arkansas.
As Rancourt et al showed in a comprehensive study, published in October 2021, that focussed on the United States, such measures continue to impact society’s most vulnerable amidst a global program of democide. The authors of the study entitled, “Nature of the COVID Era Public Health Disaster in the USA: From All-cause Mortality and Socio-geo-economic and Climatic Data”, concluded there was no pandemic and blamed “large-scale medical and government responses” for causing one million excess deaths in most vulnerable and underprivileged residents of the USA in the COVID‑era.
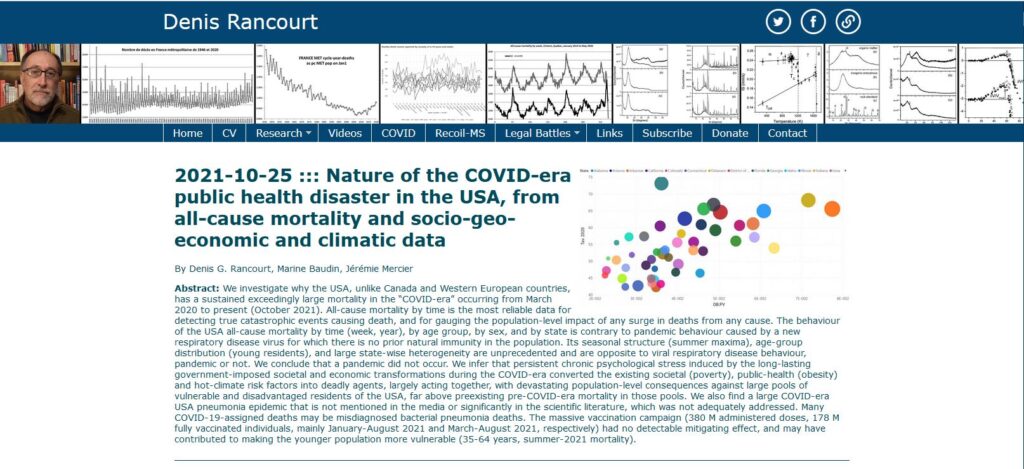
This COVID Era All Cause Mortality study found that there were two types of COVID-era deaths in the United States.
The first type was a large narrow peak occurred immediately after the WHO declaration of a ‘pandemic’. As Dr Rancourt’s first All Cause Mortality study found, this COVID peak” was caused by the aggressive novel government and medical responses that were applied in certain specific state jurisdictions, against sick elderly populations (34 states do not significantly exhibit this feature). The second type identified were peaks and excesses in the Summer of 2020, the fall-winter of 2020-2021, and the summer of 2021, which co-correlate with poverty, obesity and regional climate.
These excellent studies led by Dr Rancourt, however, do not take into account the medical democide inflicted with the use of Remdesivir.
Remarkably, as the initial ‘COVID peak’ began its decline, Redesivir came online as the FDA authorised emergency use drug to use on hospitalized Covid-19 patients. Dr Ardis says that New York’s death rate was kept high due to the Dr Fauci’s Remdesivir protocol.
➼ Anatomy of Medical Democide
These findings of Medical Democide go along way to explain why it was that once the World Health Organization declared Covid-19 a global pandemic, the cascade of events took on a warped logic belying a planet under siege of mysterious forces skilled in casting spells.
At the beginning of the Corona Pandemic, and with unseemly unity, key insiders of the global élite recast themselves as saviours of humanity while skillfully weaponizing the news with a pre-planned communications strategy designed to ‘flood the zone’ to drown-out counter-voices. The ostracization of dissenting scientists, doctors and nurses who warned that pandemic mitigation measures would cause more deaths, demolish livelihoods and transfer more wealth to the billionaire class — was a critical component to gaslight the world with fear-porn news.
The Medical Democide at the center of the ‘Corona Pandemic’ has individual, institutional, and ideological continuities with the élite Eugenics Movement — which advanced the degenerate idea of ‘hereditary hygiene’, or eliminating groups of people considered genetically inferior, as I have showed in my heretical article, “How Abortions as the Leading Cause of Death in Corona Era Reveals ‘Save the Grandmothers’ Meme to be Weaponized ironic Gaslighting”.
In a recent interview with the author of a new book, Pseudopandemic: New Normal Technocracy, Iain Davis told journalist James Corbett, that a totalitarian technocratic architecture has been built over the past two decades to consolidate power amid an engineered bio-terrorist crisis deployed with the cover-story of a planetary threatening pandemic.
This architecture for Techno-Feudalism involves fusing a global biosecurity system with carbon tax transaction system with digital central bank currencies. Such infrastrucutre is intended to extinguish privacy, free-will and ultimately — true love — since real love cannot exist without free-will, spontaneity and privacy.
The behavior modifications that have occurred so far — such as submitting to humiliating bandit mask wearing, QR-code mass surveillance, livestock swab testing, tyrannical nationwide house arrest, anti-social distancing, ‘mass vaccinations’ and ‘vaccine’ passports, as well as limitations on rights to protest, free speech, and freedom of association, Great Depression-esque long queues for food, watching Orwellian daily advisories, and World War-esque mass vaccinations — have presaged the objective to segregate society with a stealthy medical apartheid system.
In recent interviews following the publication of his book, The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health, Robert F. Kennedy Jr, said Fauci’s playbook has been to over-hype or fabricate pandemics in order to accelerate implementation of work-shopped militarized response measures, boost Big Pharma profits and set a system of totalitarian control. Kennedy describes Fauci as “the J. Edgar Hoover of public health” for his dominating, conniving and deceiving role as Director of the U.S. National Institutes of Infectious Diseases.

It turns out that Fauci has come to control the public health apparatus of the United States (and across the world) by building a network of federal fund dependent scientists, doctors and medical schools, including having 300 loyal ‘principle investigators’ to fix drug trials. Moreover, because health regulators such as FDA, NIH, CDC and WHO are largely dependent on either Big Pharma, predatory philanthropist foundations and their labyrinthine funding mechanisms, players such as Dr Fauci, Bill Gates and Robert Kadlec (among many others) have constructed a Global Health Cartel, Kennedy finds.
This biocracy, or Medical Industrial Complex, is fused with the intelligence agencies such as the CIA and MI6 through agents working on multiple foundation, university and regulatory boards, planning pandemic exercises, supervising pandemic responses and censoring credible counter-voices.
Robert F. Kennedy Jr found 17 pandemic exercises that involved hundreds of thousands of people, who were programmed to work like automated parts of a machine once a global pandemic was declared. Kennedy stated that all 17 pandemic exercises favored mass vaccinations as the primary solution. These pandemic exercises were, in fact, subversive psychic penetration rituals that served as a staging ground for sowing new hybrid narrative seeds to train (or indoctrinate) witting (or unwitting) players, attendees, and observers, as I showed in Part 3 of my series Corona World Games, entitled — All Techno-Feudalist Roads Lead to ‘Dark Winter’ Amid World’s Third Hundred Years’ War.
Kennedy also observed that border shutdowns, business closures and quarantining of the healthy were frequent pandemic script elements. Bobby Kennedy said the scenarios discounted the efficacy of existing therapeutics, avoided mention of the value of exercise, sunshine and healthy diet, or ignored the effectiveness of immunity boosting supplements.
Alas, the crucial project of identity re-codification continues to occur with subversive terminology such as ‘herd immunity’ that likens humanity to livestock. Meanwhile, a brazen re-engineering of Western Civilization occurs to extinguish liberal democracies, and replace their governance systems with technocracy.
A technocracy is an economic system that exploits technology as a means of social control through the allocation of energy and resources managed to service hidden monopolies, the privatization of government and the supreme control of unseen super-rich dynastic rulers.
The quest to reforge Western Civilization with a totalitarian bio-security matrix aims to supplant the free-will of humans by creating a totalizing planetary police state surveillance system that is intended to extinguish privacy, and therefore led to the domination of human behavior.
Absent the capacity to think freely, feel freely, and act, intuit and move freely — liberty becomes a husk marketed as commodified services. Upon this techno-tyranny trajectory, humanity is on course to be harvested as data commodities, targetted with individuated advertising mediated by social group algorithms, and automatically manipulated with bio-medical updates interfaced with the WiFi radio-wave networks.
In other words, the hyper-chip sensory world that we, the human monkeys, are being manipulated to construct, is presently on course to become a proxy for the bona fide unregulated, unmediated and un-surveilled experiences of thriving lives that are expressions of real love.
Kennedy — whose uncle was assassinated because his vision was to forge a genuine peace based on supportive co-development rather than a peace enforced by an imperial Pax Americana paradigm — warned that humanity needed to act effectively and quickly to counter the turn-key totalitarianism that is presently being fast-tracked.
To sum up, humanity is getting screwed by the degenerate global élite whom have worked out a hi-tech way to distract, divide and defeat human communities of all walks of life, with the cover-story of a global pandemic.
The gaslighting trickery seeks to re-program the majority of humanity with a combination of fear and hope, since fear scares humans with the perceived cause of the problem, while hope steers us toward the desired solutions of the global élites. It turns out that hope is the only emotion more powerful than fear. While fear is a powerful emotion to activate to control people, hope is a formiddable motivator for the long haul, to endure hardship.
However, hope is hazardous for the hierarchical rulers because if hope is abundant, such rulers will lose control of their system. Because the cosmic forces of True Love are expressive acts of positive anarchy, True Love resists regulation, fights when necessary, and creates bona fide solutions for the evolutionary rejuvenation of thriving culture.
This is not medical advice and is for informational purposes only. Any mention of dosages is for informational purposes only and not for medical use. Please consult a medical professional.
Steve ‘Snoopman’ Edwards is a dissident journalist, who worked at indigenous broadcaster, Māori Television, for 14 years as an editor of news, current affairs and general programmes. He forged his ‘Thunk Evil Without Being Evil’ super-power while writing his ground-breaking thesis on the Global Financial Crisis (GFC), titled – “It’s the financial oligarchy, stupid”– to figure out the means, modus operandi and motives of the Anglo-American Oligarchy.
Editor’s Note: If we have made any errors, please contact Steve ‘Snoopman’ Edwards, with your counter-evidence. e: steveedwards108[at]protonmail.com
Sources References:
See related report: V is for Variant Voodoo >> https://snoopman.net.nz/2022/07/04/v-is-for-variant-voodoo/

i Gilead Press Releases April 10, 2020 Data on 53 Patients Treated With Investigational Antiviral Remdesivir Through the Compassionate Use Program Published in New England Journal of Medicine. Retrieved from: https://www.gilead.com/news-and-press/press-room/press-releases/2020/4/data-on-53-patients-treated-with-investigational-antiviral-remdesivir-through-the-compassionate-use-program-published-in-new-england-journal-of-medici
ii Dr. Bryan Ardis. Retrieved from: https://thedrardisshow.com/dr-bryan-ardis
iii Lenny Bernstein, Carolyn Y. Johnson, Sarah Kaplan and Laurie McGinley (April 15, 2020). Coronavirus destroys lungs. But doctors are finding its damage in kidneys, hearts and elsewhere. Retrieved from:
https://www.washingtonpost.com/health/coronavirus-destroys-lungs-but-doctors-are-finding-its-damage-in-kidneys-hearts-and-elsewhere/2020/04/14/7ff71ee0-7db1-11ea-a3ee-13e1ae0a3571_story.html; NPR. (April 19, 2020). Shortage of Dialysis Equipment Leads to Difficult Decisions In New York ICUs. Retrieved from:
https://www.npr.org/sections/health-shots/2020/04/19/838103327/shortage-of-dialysis-equipment-leads-to-difficult-decisions-in-new-york-icus; Caitlin O’Kane (May 14, 2020). Kidney injury seen in more than a third of hospitalized COVID-19 patients https://www.cbsnews.com/news/coronavirus-patients-kidney-injury-covid-19/; Julie Steenhuysen. (May 14, 2020). Kidney injury seen in more than a third of hospitalized COVID-19 patients: U.S. study. Retrieved from: https://www.reuters.com/article/us-health-coronavirus-kidney-idUSKBN22Q0U7;
Doctors see ’unexpected and dramatic’ kidney damage from coronavirus Aug. 27, 2020. Retrieved from:
https://www.oregonlive.com/coronavirus/2020/08/doctors-see-unexpected-and-dramatic-kidney-damage-from-coronavirus.html; Aaron Feis August 3, 2020 Nearly half of coronavirus patients at NYC hospital developed kidney issues
ivNayara Aparecida de Oliveira Silva, Ana Laura de Sene Amâncio Zara, Albert Figueras, Daniela Oliveira de Melo. Potential kidney damage associated with the use of remdesivir for COVID-19: analysis of a pharmacovigilance database. DOI: 10.1590/0102-311X00077721; Anika Singh and Ashwin Kamath. (2021 Aug 5). Assessment of adverse events associated with remdesivir use for coronavirus disease 2019 using real-world data. DOI: 10.1080/14740338.2021.1962846; Jakob J Malin et al. (Dec 16 2020).Remdesivir against COVID-19 and Other Viral Diseases. Retrieved from: https://pubmed.ncbi.nlm.nih.gov/33055231/
v NIH Clinical Trial of Remdesivir to Treat COVID-19 Begins Study Enrolling Hospitalized Adults with COVID-19 in Nebraska. February 25, 2020. Retrieved from: https://www.niaid.nih.gov/news-events/nih-clinical-trial-remdesivir-treat-covid-19-begins
vi NIH Clinical Trial Shows Remdesivir Accelerates Recovery from Advanced COVID-19
April 29, 2020 https://www.niaid.nih.gov/news-events/nih-clinical-trial-shows-remdesivir-accelerates-recovery-advanced-covid-19
vii Nicole Darrah. (Apr 29 2020). POSITIVE DIAGNOSIS Dr Fauci hails remdesivir as a ‘drug that can block coronavirus’ as FDA in talks to get antiviral to patients quickly https://www.the-sun.com/news/755584/coronavirus-drug-cure-remdesivir-recover-quickly/; April 29, 2020 Fauci on remdesivir for COVID-19: ‘This will be the standard of care’
viiiDr. Ardis Interview – Death By Remdesivir: The Illusion Lynchpin Of COVID-19 Risk. Retrieved from: https://www.thelastamericanvagabond.com/dr-ardis-interview-death-by-remdesivir-illusion-lynchpin-covid-19-risk
ix Alexandre O. Gérard et al. (19 December 2020). Remdesivir and Acute Renal Failure: A Potential Safety Signal From Disproportionality Analysis of the WHO Safety Database. Retrieved from https://doi.org/10.1002/cpt.2145
x UNC-Chapel Hill (April 29, 2020). Remdesivir, developed through a UNC-Chapel Hill partnership, proves effective against COVID-19 in NIAID human clinical trials
xii John H. Beigel, M.D et al. (October 8, 2020). Remdesivir for the Treatment of Covid-19 — Final Report. Retrieved from: https://www.nejm.org/doi/full/10.1056/NEJMoa2007764; Adaptive COVID-19 Treatment Trial (ACTT). Retrieved from: https://clinicaltrials.gov/ct2/show/NCT04280705
xiiiDoctors for Covid Ethics Symposium. UK Column News. https://doctors4covidethics.org/symposium/; 8 Prominent Doctors & Scientists Engage in Remarkable Exchange Covid Pandemic Panel [23 September 2021, San Juan Puerto Rico] https://3speak.tv/watch?v=pandemichealth%2Fraukfhng
xivDr. Brian Ardis warns America approaching ONE MILLION DEATHS from remdesivir and ventilator homicide https://www.brighteon.com/786597c9-0c4d-4d0a-9c28-dd94395c29e1; Brian P. Dunleavy. (March 23, 2020). New York launches new COVID-19 drug trials; more underway in China. https://www.upi.com/Health_News/2020/03/23/New-York-launches-new-COVID-19-drug-trials-more-underway-in-China/3681584975924/
xvNational Institutes of Health (NIH). (July 8, 2021 ). Remdesivir. Table 2e. Characteristics of Antiviral Agents That Are Approved or Under Evaluation for the Treatment of COVID-19 https://www.covid19treatmentguidelines.nih.gov/tables/table-2e/
xvi Remdesivir (Veklury) [package insert]. Food and Drug Administration. 2020. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/214787Orig1s000lbl.pdf
xviiWHO Solidarity trial consortium, Hongchao Pan, Richard Peto, Quarraisha Abdool Karim, Marissa Alejandria, Ana Maria Henao-Restrepo, César Hernández García, Marie-Paule Kieny, Reza Malekzadeh, Srinivas Murthy, Marie-Pierre Preziosi, Srinath Reddy, Mirta Roses Periago, Vasee Sathiyamoorthy, John-Arne Røttingen, Soumya Swaminathan, as the members of the Writing Committee. Repurposed antiviral drugs for COVID-19 –interim WHO SOLIDARITY trial results
https://www.medrxiv.org/content/10.1101/2020.10.15.20209817v1/ doi: https://doi.org/10.1101/2020.10.15.20209817
Plant-Derived Natural Non-Nucleoside Analog Inhibitors (NNAIs) against RNA-Dependent RNA Polymerase Complex (nsp7/nsp8/nsp12) of SARS-CoV-2 Sreus A. G. Naidu ORCID Icon, Ghulam Mustafa ORCID Icon, Roger A. Clemens ORCID Icon & A. Satyanarayan Naidu ORCID Icon Published online: 01 Dec 2021 Download citation https://doi.org/10.1080/19390211.2021.2006387 CrossMark Logo CrossMark https://www.tandfonline.com/doi/abs/10.1080/19390211.2021.2006387?journalCode=ijds20
xviii Federal Register. (6 Novemeber 2020). Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency. Retrieved from: https://www.federalregister.gov/documents/2020/11/06/2020-24332/additional-policy-and-regulatory-revisions-in-response-to-the-covid-19-public-health-emergency
xix Charles Creitz. (April 9, 2020). Minnesota doctor blasts ‘ridiculous’ CDC coronavirus death count guidelines. Fox News. https://www.foxnews.com/media/physician-blasts-cdc-coronavirus-death-count-guidelines
xx Larry Levitt, Karyn Schwartz, and Eric Lopez. (Apr 07, 2020). Estimated Cost of Treating the Uninsured Hospitalized with COVID-19. Retrieved from: https://www.kff.org/uninsured/issue-brief/estimated-cost-of-treating-the-uninsured-hospitalized-with-covid-19/
xxiNational Center for Health Statistics. (April 2020). “Certifying deaths due to COVID-19.” Vital Statistics Reporting Guidance Report No. 3 ▪ April 2020 Guidance for Certifying Deaths Due to Coronavirus Disease 2019 (COVID–19). U.S. Department of Health and Human Services • Centers for Disease Control and Prevention • National Center for Health Statistics • National Vital Statistics System. Retrieved from: https://www.cdc.gov/nchs/data/nvss/vsrg/vsrg03-508.pdf
xxiiThe Spectator. April 9, 2020. Hospitals Get Paid More to List Patients as COVID-19 and Three Times as Much if the Patient Goes on Ventilator (VIDEO). https://thespectator.info/2020/04/09/hospitals-get-paid-more-to-list-patients-as-covid-19-and-three-times-as-much-if-the-patient-goes-on-ventilator-video/?utm_source=wnd&utm_medium=wnd&utm_campaign=syndicated
xxiii First large-scale study links acute kidney injury and COVID-19 hospitalizations Matthew Libassi May 14th, 2020
https://feinstein.northwell.edu/news/the-latest/first-large-scale-study-links-acute-kidney-injury-and-covid-19-hospitalizations; Kidney International https://www.kidney-international.org/article/S0085-2538(20)30532-9/fulltext; Robert Preidt. (May 11, 2020). Kidney Failure Often a COVID-19 Complication. HealthDay.
Veklury (remdesivir) ASPR’s Portfolio of COVID-19 Medical Countermeasures Made Available as a Licensed Product. Office of the Assistant Secretary for Preparedness and Response. U.S. Department of Health and Human Services. Retrieved from: https://www.phe.gov/emergency/events/COVID19/investigation-MCM/Pages/Veklury.aspx
Sainath Suryanarayanan. (February 15, 2021). Emails show scientists discussed masking their involvement in key journal letter on Covid origins. https://usrtk.org/biohazards-blog/scientists-masked-involvement-in-lancet-letter-on-covid-origin/
Gilead Sciences Announces Veklury® Donations to Help Address the Ongoing COVID-19 Crisis in Indonesia and Armenia October 20, 2021 >> https://finance.yahoo.com/news/gilead-sciences-announces-veklury-donations-123000217.html